Introduction
The intravenous (IV) route for antimicrobial therapy is commonly utilized for patients hospitalized with infections because of higher and faster peak serum concentrations in comparison to the oral (PO) route. Although IV therapy provides a pharmacokinetic benefit, it carries risks such as phlebitis, thrombosis, extravasation, and infections and PO antibiotics are clinically effective.1 Switching to PO therapy in the hospital has been associated with shorter length of stay, increased patient satisfaction, and cost savings.1–4 To realize these benefits, many institutions develop IV to PO switch practices to support medication route conversion for patients meeting certain clinical parameters. This is often done by clinical pharmacists.5 The IV to PO switch practices may be outlined in the form of a protocol or a guideline. An IV to PO protocol is a policy which allows the switch to occur in a patient meeting pre-specified criteria without an explicit provider order. In contrast, a guideline is a document which gives recommendations or best practices regarding IV to PO switch, but requires a discussion of the recommendation with a provider and provider approval is necessary to change the medication route. Various institutions across the state of Kentucky have implemented robust IV to PO switch practices; however, numerous facilities currently operate with minimal or no IV to PO switch guidance. Hospitals may benefit from a review of IV to PO switch practices at institutions in Kentucky, and ultimately use this to enhance current practice or create new guidelines or protocols. The purpose of this document is to summarize IV to PO switch practices utilized by healthcare institutions with established antimicrobial stewardship programs across Kentucky.
Methods
The Kentucky Antimicrobial Stewardship Innovation Consortium (KASIC) strives to improve antibiotic use across Kentucky and includes an Advisory Board which consists of pharmacists who practice in established antimicrobial stewardship programs at their institutions. KASIC invited the Advisory Board to share their current IV to PO switch practices. The documents were evaluated in a systematic approach and the information was collated to demonstrate similarities and differences.
Results
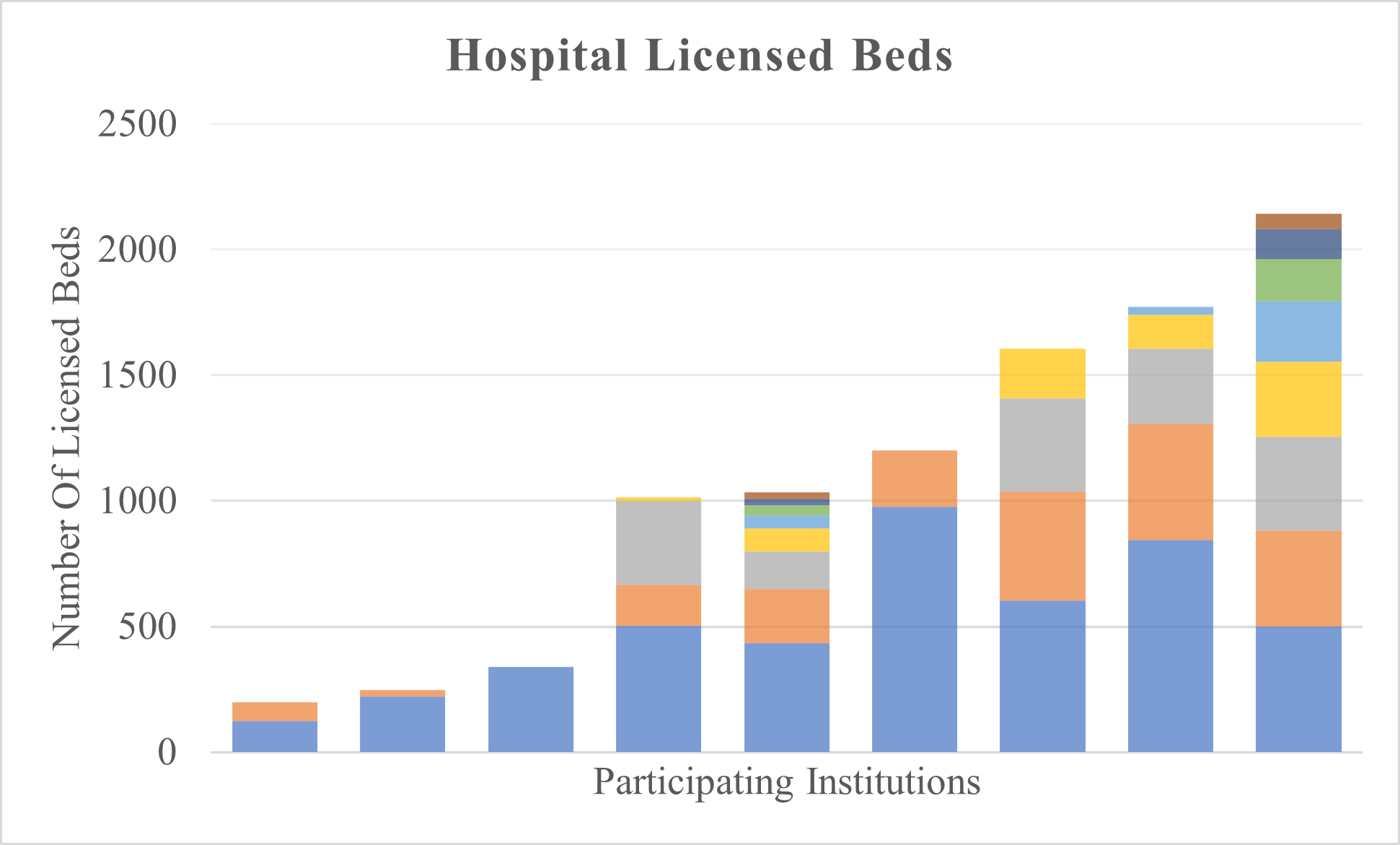
Nine of the ten institutions represented by the Advisory Board submitted their IV to PO switch practices for analysis. The Appendix contains the submitted documents in an abbreviated format which includes only sections relevant to antimicrobials. The protocols in the Appendix are listed in no particular order. There was substantial variation in the characteristics of institutions that submitted their documents. The types of institutions included community hospitals, academic medical centers, and long-term acute care hospitals. Additionally, some protocols submitted were utilized by large health systems that included more than one hospital. The number of licensed beds of contributing hospitals ranged from approximately 100 beds to more than 800 beds (Figure 1).

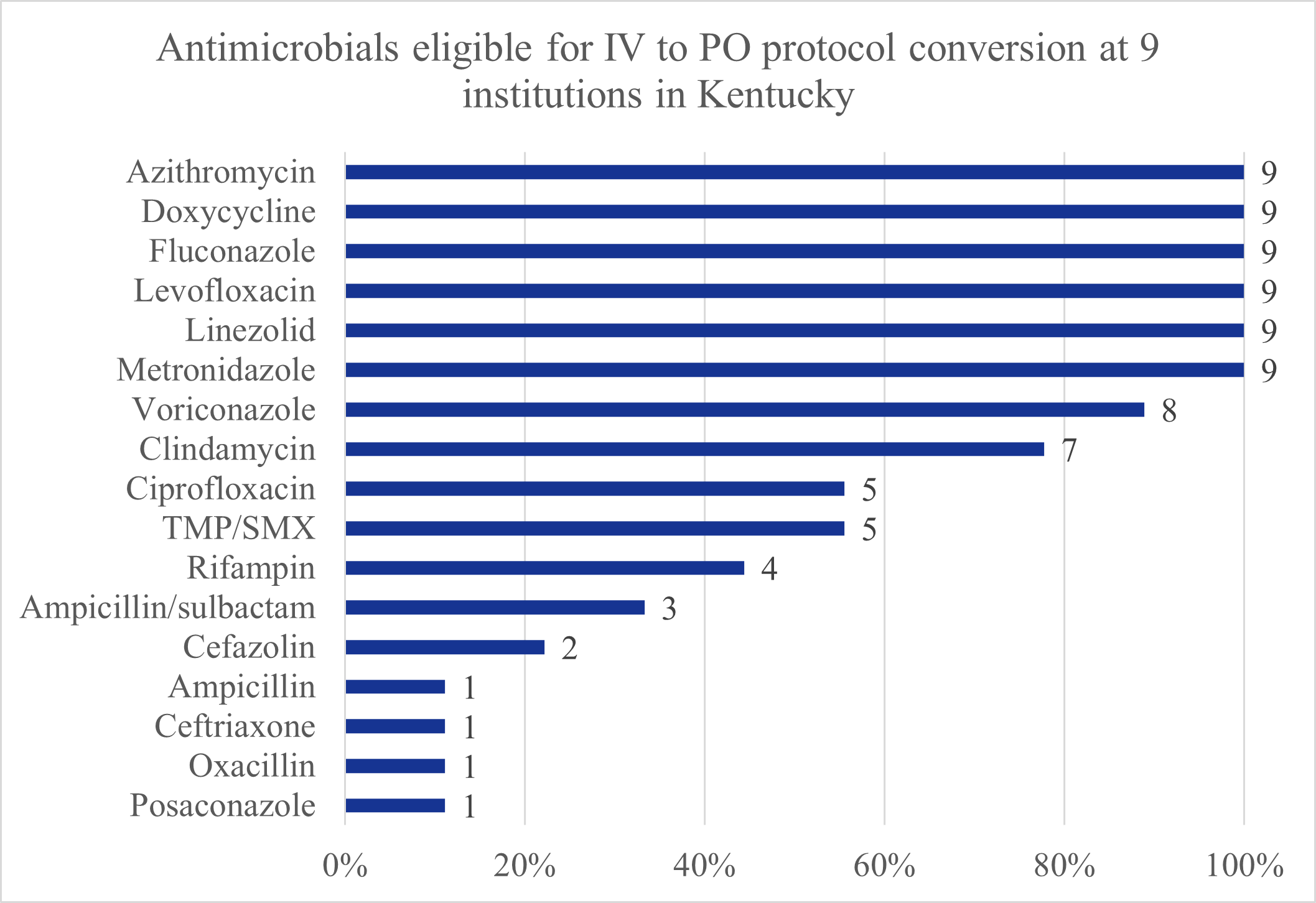
All institutions utilized protocols which gave pharmacists authority to convert antimicrobial therapy from IV to PO without a provider order if pre-specified criteria outlined in the protocol were met. Protocols differed in terms of which antimicrobials were eligible for conversion and the criteria required for conversions to occur. Specific antimicrobials eligible for conversion at institutions are shown in Figure 2. Of note, some protocols included conversion of antimicrobials that involved different drugs for the IV and PO counterparts, namely within the β-lactam class of antibiotics. This included IV ampicillin/sulbactam to PO amoxicillin/clavulanate, IV ampicillin to PO amoxicillin, IV oxacillin to PO dicloxacillin, IV cefazolin to PO cephalexin, and IV ceftriaxone to PO cefdinir.

The protocols varied in the level of guidance provided for implementation of conversions, specifically regarding conversion doses and ratio/bioavailability information. Four of nine (44%) institutions had both conversion doses and ratio/bioavailability information listed in the protocol, two of nine (22%) had one of these pieces of information, and 3/9 (33%) had neither.
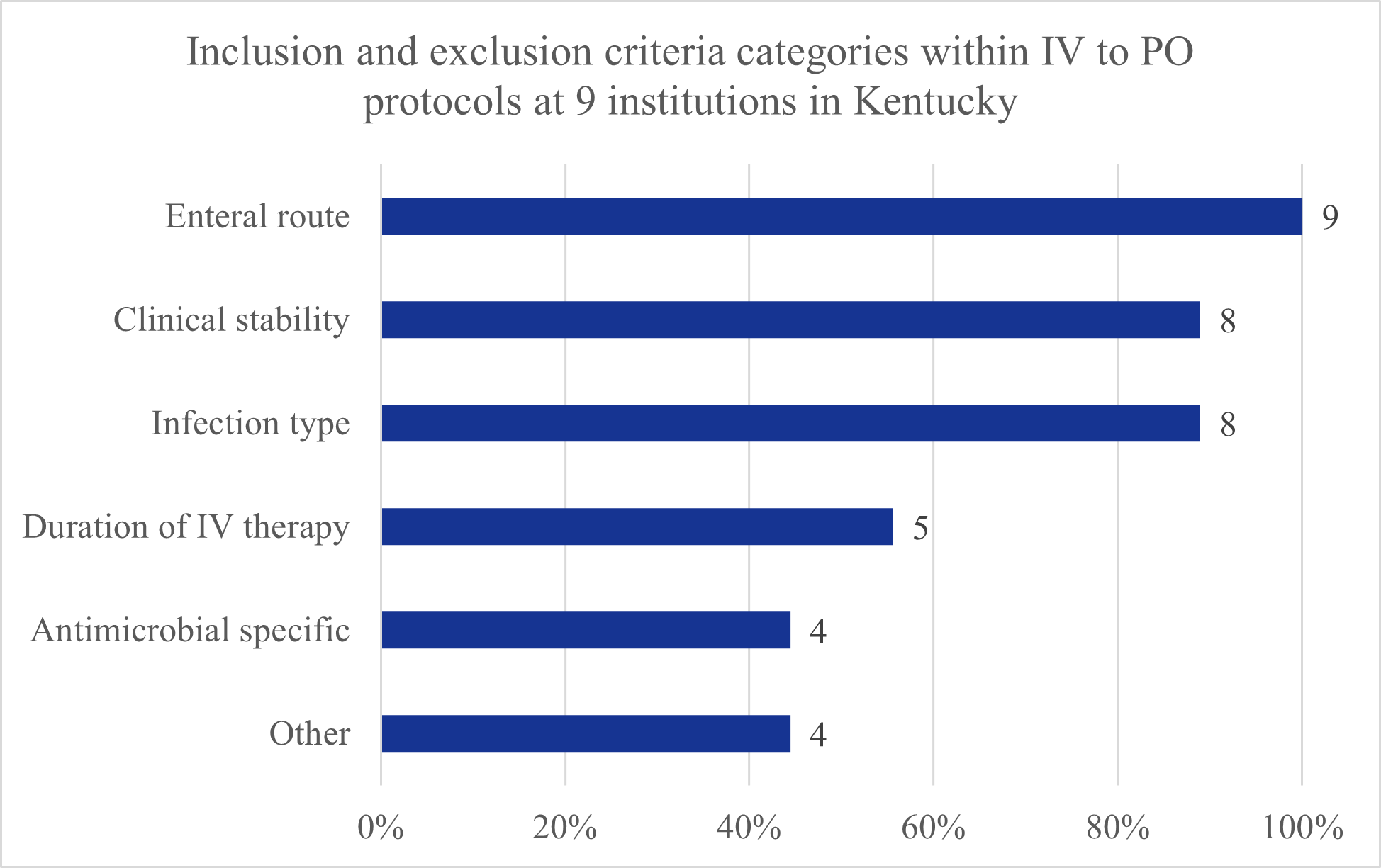
Each protocol listed either inclusion criteria, exclusion criteria, or both. The most common consideration was related to patients’ ability to receive medications via the enteral route (taking other PO medications, tolerating diet, etc). Other criteria such as clinical stability or infection type were addressed by some, but not all of the protocols (Figure 3). Table 1 lists all the specific inclusion and exclusion criteria identified in the protocols by category. There were many variations within each criteria category, particularly for enteral route, clinical stability, and infection type categories. Table 2 shows antimicrobial specific criteria that must be met in order for that particular antimicrobial to be eligible for conversion (in addition to other criteria). Overall, there was little variation in the antimicrobial specific criteria themselves among institutions. For example, concomitant tube feeding was the only exclusion criteria listed for IV doxycycline in protocols that specified additional criteria for this antimicrobial. The various combinations of inclusion and exclusion criteria utilized by each protocol are shown in the Appendix.

Discussion
This review identified that most institutions with established antimicrobial stewardship programs in Kentucky have IV to PO protocols, which are implemented by pharmacists per protocol without a specific order from a provider. The contents of the protocols differed by the type of antimicrobials eligible for conversion, clinical eligibility criteria, and level of guidance provided for implementation of the protocol.
There were several antimicrobials which all institutions had on their respective IV to PO protocols (Figure 2). However, others were not universally represented. Reasons for this may include niche indications/low utility (e.g. posaconazole) or lack of direct equivalent PO option (e.g. ampicillin/sulbactam). Switching from an IV formulation to PO of the same antibiotic is fairly straight forward once the correct dose is chosen. However, it is notable that several institutions allow for conversion of certain IV agents which do not have an equivalent PO formulation or do not have a PO formulation with adequate bioavailability. In these cases, the conversion is performed to a PO agent within the same class as the IV agent. Caution should be used since route conversion may not result in equivalent antibiotic exposure. An example of this would be conversion from IV ceftriaxone to PO cefdinir, which has an estimated oral bioavailability of only up to 25%.6 Care should be taken when determining which patients are eligible for such conversions and the decision should take into account infection source and severity. In the future, this practice may pave the way to more innovative ways to perform routine IV to PO conversions, such as inter-class switch to an agent with a similar spectrum of activity or perhaps even de-escalation of spectrum in select patients.
The majority of institutions provided guidance on dose or IV to PO conversion ratios to be used when switching patients. Having this information readily accessible allows pharmacists to appropriately convert IV antimicrobials to the equivalent PO formulation. This is particularly relevant for antimicrobials which do not have one to one conversion or require transitioning from a weight-based dose to fixed dose.
Another important aspect of IV to PO protocols is determining which patients may be appropriately switched. No protocol was alike in terms of the specific inclusion and exclusion criteria used to identify patients who are appropriate for a switch. Some institutions were more specific and restrictive than others. The authors did not attempt to develop best practices for IV to PO protocols within the scope of this manuscript given that local prescribing culture heavily influences what type of IV to PO switch strategy may be viable. The optimal eligibility criteria are typically chosen based on a consensus from an institution’s clinical leadership and feasibility of implementation of such criteria.
This review serves to disseminate information on IV to PO switch practices utilized by institutions with established antimicrobial stewardship programs in Kentucky. Although the adherence rates to the protocols and associated outcomes are unknown, this summary provides a starting point for institutions seeking to start an IV to PO program or enhance an existing program. IV to PO switch practices should be tailored to the institution’s needs, clinical decision-making culture, and feasibility.