BACKGROUND
The COVID-19 pandemic has underscored the pivotal role of vaccination in preventing severe illness, hospitalization, and fatalities resulting from SARS-CoV-2 infection.1 This virus has disproportionately impacted minority communities, revealing a stark disparity in vaccination rates.1,2 The COVID-19 pandemic has worsened existing disparities in the United States in terms of race, social status, and economic conditions. This has resulted in greater risk of exposure to the SARS-CoV-2 virus, limited access to protective resources, disparities in illness and increased death rates among individuals living in low-income neighborhoods, indigenous populations, and communities with predominantly non-white populations.1,2 Vaccine hesitancy stemming from mistrust of vaccine safety information and skepticism regarding traditional vaccination procedures has further exacerbated lower vaccination rates and higher COVID-19 hospitalization rates among non-white populations.1,3
Addressing these disparities necessitates a comprehensive strategy that not only makes vaccines readily accessible but also forges partnerships with trusted local entities capable of engaging with targeted communities. In Louisville, Kentucky, initial COVID-19 vaccination efforts focused on mass immunization through the LouVax-Broadbent, a community drive-through mass immunization effort held at Broadbent Area, designed to serve large segments of the population.4 As part of this effort, there was a need to transition from mass vaccination to targeted vaccination within communities at higher risk for disease transmission or where vaccine hesitancy prevailed. To tackle these challenges of access and acceptance, the transition to a mobile vaccination approach was initiated, acknowledging the barriers faced by vulnerable populations and the importance of reaching communities most in need, often with the assistance of trusted community leaders. Strengthening vaccine confidence while removing structural barriers to access are imperative to ensuring that all residents benefit from vaccination.2
The agility and adaptability of mobile vaccination clinics made them an ideal solution for addressing the unique needs of various communities during the COVID-19 pandemic. The Louisville Metro Department of Public Health and Wellness identified areas with low vaccination rates and documented COVID-19 cases, which served as the foundation for a community-centric mobile vaccination outreach plan. Local leaders and organizations provided valuable guidance in the development of this plan. The final hurdle in this transformative process was establishing a safe and sustainable mobile vaccination infrastructure. This paper aims to achieve the following objectives:
1) Describe the planning process behind the transition from mass immunization to LouVax-Mobile vaccination clinics, building upon the success of the public health and volunteer workforce that made LouVax-Broadbent mass drive-through immunization initiative effective; 2) Outline the comprehensive training program implemented to ensure the safe deployment of COVID-19 mobile vaccination clinics across the Louisville, Kentucky, metropolitan area; 3) Discuss the challenges encountered during the implementation of mobile vaccination clinics amidst the dynamic landscape of a pandemic.
METHODS
Planning for LouVax-Mobile vaccination clinics
Planning for LouVax-Mobile vaccination clinics began in late winter 2020 and early spring of 2021. By that time, more than 100,000 doses of vaccine had been administered through the initial mass immunization site, LouVax-Broadbent.4 This provided an opportunity to shift from the large drive-through mass vaccination events to a community-based outreach effort using a mobile vaccination approach. The multidisciplinary planning team consisted of researchers, clinicians, epidemiologists, infection preventionists, information technologists, and emergency preparedness personnel from the University of Louisville, Kentucky Nurses Association (KNA), and a host of planners at the Louisville Metro Department of Public Health and Wellness (LMPHW), all with experience in mass immunization. Planning objectives included: 1) engagement of key partners in targeted areas of the community; 2) outlining the logistical operations for the mobile clinic; 3) enlisting, training, and verifying the competence of the volunteers; 4) clinic operations and patient throughput; and 5) operational and financial evaluation.
Engagement of Key Partners
As was learned during mass immunization events, it was vital that the vaccination approach be centered on partners from within the targeted areas of the community. Identification of individuals and organizations with credible and trusted ties to the local community helped engage individuals, identify suitable sites for the mobile clinics, and provide important capabilities (e.g., interpreters), making the events a success. Members from the KNA held more than fifty ‘listening sessions’ to help identify local immunization champions and garner interest and support for the clinics. These sessions helped move the concept of LouVax mobile vaccination clinics from a public health clinic to one that was ‘owned’ by the local community. In terms of support and access to the local population, time and effort spent on key partner engagement was a pivotal part of the planning process.
Logistical Operations
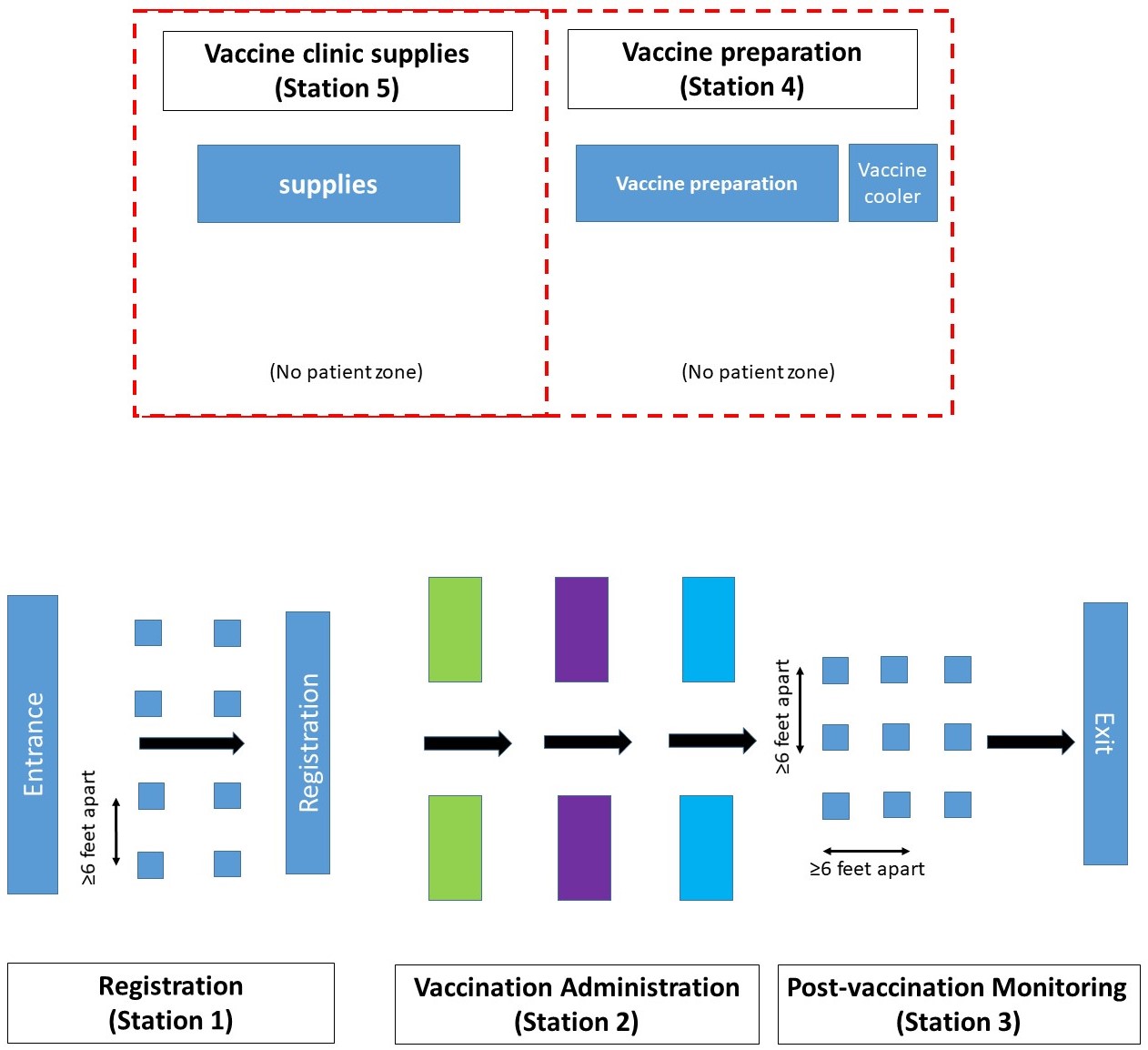
An operations manual was one of the first documents developed for LouVax- Mobile vaccination clinics, outlining the entire process, including initial site visits, supply lists, vaccine and supply delivery processes, workflow and patient throughput, data collection, and data entry. Lessons learned from the LouVax-Broadbent were valuable in developing this initial manual. Site visits were key to successful operations. Site visits were conducted at least a week prior to the vaccine event by the health department lead or a KNA representative to assess the site for an adequate environment, workflow and patient throughput, staffing, and allotment of supplies for each clinic. Clinics were held in outdoor or indoor settings such as local outpatient offices, parking lots, libraries, halfway homes, adult daycares, gyms, dialysis centers, churches, and other community and faith-based organizations. Sites were evaluated for areas with the potential for stagnant airflow, and clinics were organized to allow for open doors and windows to promote ventilation and air dilution. Masks were required for all clinic personnel and patients throughout all vaccination events. LouVax-Mobile clinics were also conveniently located at walk-through and handicap-accessible sites. During site visits, stations were identified for registration (station 1), vaccine administration (station 2), post-vaccination monitoring (station 3), vaccine preparation (station 4), and Vaccine clinic supplies (station 5). This helped map the flow of the clinic and maximize capabilities while minimizing the structural challenges of the site. Figure 1 shows a diagram of the mobile vaccination clinic flow. LouVax-Mobile vaccination sites were required to have accessible bathrooms and handwashing facilities, adequate or adjustable site temperatures for vaccine protection, functional power outlets for vaccine coolers and laptops, and parking areas for staff, volunteers, and those seeking vaccination. Based on the size of the location and the anticipated number of doses to administer, supply lists were developed, and health department personnel were responsible for gathering and delivering supplies. Vaccine doses were also obtained from the health department, and immunization program personnel gathered the vaccine, packed it for transport, and delivered the vaccine to the site. Assistance from the health department was invaluable as they stayed with supplies and vaccines, monitored the vaccine for temperature maintenance, completed documentation regarding doses administered, and transported unused vaccines back to the health department for storage. Health department information technology (IT) personnel were also on-site to enter vaccination information into the state’s immunization registry, the Kentucky Immunization Registry (KYIR). This process helped clearly delineate responsibilities for the mobile clinics. The operations side, including the preparation and transport of supplies and vaccines, data entry, and site security, were managed by health department personnel, and all activities involving the handling and administering of the vaccine, documentation, and post-vaccination monitoring were the responsibility of the KNA Team Leaders and volunteer staff.

Enlisting, Training, and Competence of the Vaccinating Workforce
A unique aspect of the LouVax-Mobile vaccination clinics was the ability to tap into underutilized community resources in the form of volunteers for the vaccinating workforce. The process of identifying, engaging, and training a full spectrum of healthcare workers as well as clerical volunteers had been the basis for the successful LouVax-Broadbent mass immunization process. Therefore, it was a natural process to transition the volunteer workforce from mass immunization to mobile clinic operations. Volunteer healthcare workers continued to be recruited through professional associations such as the KNA, while clinical and nonclinical volunteers could also sign up directly through the LMPHW volunteer website. LouVax-Mobile clinics also served as a clinical site where nursing students from local colleges could participate with clinical sites under the direct supervision of their school faculty. Community partners often provided additional volunteers and certified medical translators to assist with consent completion and patient education, thereby enhancing the influence and engagement of local champions. By utilizing community partners and nurses as the main clinic staff, barriers such as mistrust from the community of vaccination by local government agencies were minimized.
An Advanced Practice Registered Nurse with expertise in immunization, infection control, education, performance improvement, management, and leadership served as the clinical nurse Team Leader for LouVax-Mobile clinic operations. A clinical Team Leader was also responsible for the operational efficiency and safety of the vaccination event. This Team Leader assigned roles, trained, and oriented volunteers to their roles prior to beginning their shift. All volunteers were trained at each session, without exception. Aspects of training were focused on the competencies required for each role. Training procedures, operations manuals, tools, and resources for training were developed by a small team from the Kentucky Infection Prevention Training Center (University of Louisville and Norton Healthcare) and updated frequently as part of continuous performance assessment and quality improvement. The standard operating procedures and training manual for LouVax-Mobile vaccination clinics is available in the supplemental materials. Competency-based and standardized training with a return demonstration was provided for every volunteer before the staffing event. Ongoing training engages new Team Leaders and volunteers and sharpens the competencies of existing Team leaders and volunteers.5 Licensed volunteers (e.g., Registered Nurses, Registered Pharmacists, Physicians) were responsible for vaccine preparation, administration, and post-vaccination monitoring. Nonclinical volunteers were assigned roles such as registration, vaccinator helpers (e.g., helping complete CDC vaccination cards, communicating with IT personnel regarding prior vaccination questions), and vaccine runners. Like LouVax-Broadbent mass immunization operations, training had three overarching goals: to protect the vaccine supply, to protect the individuals being vaccinated, and to protect the healthcare workforce involved in the process.4
Training effectiveness was evaluated by observing the volunteer’s skills during the clinic and by obtaining feedback from volunteers during post-clinic debrief. Comments obtained during the post-vaccination event debrief were used to improve processes. Additional items were developed for vaccine providers including color-coded graphics of vaccines, vaccine doses, and timing; improved signage to assist with throughput; activities for children waiting for vaccination or with family members; privacy areas to address cultural concerns during vaccination; and a process to quickly obtain additional vaccines or supplies if need outpaced supply. All these processes required constant training of volunteers.
Patient Throughput
Individuals coming to the site for vaccination began the process at a registration table [Figure 1]. There, a blank personal encounter form was completed for the primary series or booster doses. Registration personnel verified the patient’s date of birth and the legibility of the encounter form. A parent or legal guardian had to be present to complete and sign the encounter form before a minor could proceed to the vaccination station. If a legal guardian was not physically present for children aged 12 to 18 years, telephone consent could be obtained by the licensed healthcare professional administering the vaccine and a witness. Other responsibilities of registration personnel involved reviewing the encounter form to ensure that all sections were completed, signed, and that the writing was legible, as this directly impacted what the information technology personnel could enter KYIR, or what they could gather in the event prior vaccination history was needed. Record-keeping was particularly challenging for vaccine recipients who had more than one last name. All names had to be listed on the encounter form and written in the order that they appeared on their official identification documentation (e.g., drivers’ license, utility bill). The encounter forms were reviewed by a healthcare provider at the vaccination station as a final check for completion, legibility, birthdate verification, contraindications to vaccination, and vaccination history.
Patient education began as soon as the individual arrived, beginning at the time of registration. Once individuals were inside the vaccination site, they were provided with a hard copy of the Emergency Use Authorization vaccine fact sheet (either from Pfizer, Moderna, or Janssen). Patient education was provided, outlining the differences between expected immune responses such as fever, myalgia, malaise, headache, and adverse events. Information on how to report adverse events and how to treat expected immune responses was made available. For convenience and trust building, all vaccination clinics were walk-in and did not require an appointment. Any questions or concerns from community members regarding the vaccine were immediately addressed by the clinical Team Leader onsite. This helped provide confidence in vaccines and debunk myths fueling reluctance and mistrust within the community.
Due to the diverse population served during each clinic, encounter forms, vaccine information statements, and any handouts (e.g., HIPAA forms and follow-up vaccination clinic schedules) were available in six languages. These languages were Somali, Amharic, Arabic, Tagalog, Spanish, and English. Onsite medical interpreters were provided by the Louisville Metro’s Office of Globalization, Catholic Charities, Family Health Center and other community partners. Sign-language interpreters and language interpreter services were available as needed. Only certified medical interpreters were authorized to interpret protected health information. Interpreters provided by the hosting organization or company could not assist with interpreting screening questions but were invaluable in helping direct patients to vaccination or waiting areas, answering general questions, and establishing a welcoming and trustworthy environment.
Vaccination occurred at specific vaccination stations. The number of vaccination stations was dependent on the anticipated number of vaccine recipients at each clinic. Each vaccination table had two volunteer personnel: one licensed healthcare worker trained to administer intramuscular vaccination and one person responsible for completing the CDC vaccination card and ensuring completion of the encounter form. Patient data was entered into KYIR and the additional database used by LMPHW information technology (IT) personnel (SalesForce Inc., San Francisco, CA). This enabled the maintenance of local vaccination data for program impact and financial monitoring. Vaccine recipients were called individually to the vaccination station unless they were a family. The vaccinator verified the vaccine recipient’s date of birth, age, contraindications to vaccination, and dosing of the vaccine prior to vaccinating. Vaccine recipients were immunized with the vaccine type and dosage according to their age on that date. Manuals outlining the vaccination process were updated in real-time to incorporate vaccine expansions to additional age groups, such as children, and updates to booster dosing recommendations. For those who reported for vaccination but did not have their CDC vaccination card, information technology personnel were able to access data in KYIR to verify prior doses.
Vaccine transport and storage
All vaccines and supplies were delivered to the mobile site by LMPHW personnel using vaccine-grade transport refrigerators accompanied by data loggers for temperature monitoring. A designated LMPHW transporter remained with the vaccine cooler during the entire clinic and completed the hourly vaccine cooler temperature monitoring log as standard practice. The vaccine cooler containing the vaccine was never left unattended to ensure the safety of the vaccine. Prior to the session, the Team Leader verified that the vaccine cooler was plugged into a functioning power outlet and noted the vaccine type, number of doses received, vaccine lot number, and expiration date on each vaccine vial. This information was verified and compared to the stickers containing vaccine information that were placed on the CDC vaccine card. When all the information matched, the stickers were distributed to the appropriate vaccination stations. Transport refrigerators contained a single type of vaccine from a single lot. If multiple lots or vaccine types were delivered, they would be in a separate transport refrigerator and remain separated throughout the vaccine event day. Due to a constantly changing environment at each clinic, ambient temperatures were monitored to ensure that prepared doses of vaccine were not subjected to unfavorable or harsh temperatures that would negatively affect the integrity of the vaccine.
Vaccine Preparation
The difference in vaccine dosages, dilution processes, and preparation coordination made vaccine preparation a particularly challenging process that required a more focused approach and diligence. To facilitate efficiency, the preparation process was divided into multiple steps, with personnel assigned specific responsibilities. Individuals responsible for vaccine preparation (vaccine preparation area) reviewed the vaccination preparation guide resource prior to beginning vaccine preparation. Prior to vaccine preparation, table surfaces were disinfected, and hand hygiene was performed. Syringe and needle packages were opened and managed in a way that prevented contamination or touching of the sterile areas of those items. The needle was immediately connected to syringes when packages were opened. Prepared syringes were placed on a dental bib in preparation for filling. When filled, syringes were placed into plastic storage containers, where the Team Leader would assess each filled syringe prior to distribution to the vaccine tables. Unfilled syringes were not stored in plastic containers to prevent inadvertently sending unfilled syringes to the vaccination table. The clinical Team Leader for the individual clinic site reviewed techniques and observed dilution (if needed) and techniques for syringe preparation and filling prior to the first doses of vaccine being released to the vaccination tables.
Reducing Vaccine Errors
Major focus was placed on reducing vaccination errors. Team Leaders received training prior to the vaccination event, and volunteers received orientation and training at the start of each vaccination clinic. Not every member of the healthcare staff could exhibit proficiency in the procedures required for accurately withdrawing vaccine doses into syringes or for safely diluting the vaccine. This deficiency emerged as a significant focus for training and competency assessment. It was apparent that the existing practices in healthcare settings primarily entrusted the preparation of medication doses to pharmacy personnel. Consequently, physicians and nurses frequently encountered difficulties when it came to filling syringes with the appropriate volumes and applying infection control methods based on evidence.4 Vaccine protective activities included: 1) checking the expiration dates of the vaccine; 2) monitoring the temperature and environmental conditions of the vaccine throughout the preparation and dilution processes; 3) selection and use of appropriate needle and syringe combinations for preparation and administration; 4) drawing up all doses from a reconstituted vial or a ready-to-use vial before distributing it to vaccination stations with verification of dose volume, 5) procedures to prepare vaccine so that each syringe was ready for injection, 6) labeling and delivering syringes to the vaccination table, 7) controlled maintenance of the filled syringes through delivery to the vaccination stations and until administration to the vaccine recipient, 8) monitoring of time between vaccine vial removal from the refrigerated environment and vaccine administration, and 9) utilizing color-coded visual cues to differentiate between various vaccine types and doses (e.g., purple assigned to all vaccines involving Pfizer product [for adults] or orange [for children]; blue and red for Moderna vaccine). During a vaccination event where multiple vaccine types, doses, and formulations were present, vaccine safety was enhanced by color-coding syringe labels, tablecloths, stickers for the CDC vaccination cards, and encounter form labels. This was also done to clearly separate the adult from the pediatric doses, as with the Pfizer vaccine, or when there was a difference in dosages between the primary series and booster doses, as seen with Moderna.
Protecting the Vaccine Recipient
Protecting the vaccine recipient required that the process: 1) uniformly screen all recipients prior to vaccination; 2) ensure infection prevention and control throughout the vaccination process; 3) ensure safe injection practice; 4) use administration techniques to facilitate intramuscular injection of the vaccine; 5) document the screening and vaccination process; 6) recognize and respond to immediate adverse events; and 7) provide patient education, including orientation to CDC V-safe guidelines. Regardless of how frequently an individual had participated in mobile vaccination clinics, standardized training procedures were developed, and group training for all personnel was conducted during each vaccination clinic.
Post-vaccination monitoring
Personnel that were certified in basic life support and trained in recognizing adverse reactions to vaccines and administering epinephrine were assigned to the post-vaccination waiting area. Anaphylaxis protocols and an emergency medical kit containing adult and pediatric epinephrine auto-injectors and liquid diphenhydramine were kept readily available during each clinic. Medication expiration dates were checked at the beginning of the vaccination session. If the patient exhibited or complained of physical symptoms (e.g., itching, numbness or tingling, breathing complaints, or changes in behavior such as restlessness), the clinical Team Lead was notified to assess the patient. Special attention was given to vaccinated children as they may rapidly progress from mild to severe symptoms of distress. The clinical Team Leader was trained to notify EMS and local police as deemed necessary in case of an emergency.
Protecting the Vaccine Administration Workforce
Ensuring the safety of all personnel involved in vaccine administration was embedded throughout the entire process, beginning with standardized training for all personnel regarding infection prevention and control practices, sharps safety, selection, and use of personal protective equipment (PPE), and continuous process monitoring for performance improvement. All personnel were required to always wear a medical grade face mask, even when masking policies were relaxed by the CDC or the local health department. Masks were also available at the registration area for individuals coming for vaccination, including those accompanying friends or family members. Food and drink, other than bottled water, were prohibited at the vaccination tables to minimize mask removal. Training included a review of infection control basics such as hand hygiene, safe injection practices, syringe and needle review emphasizing safety devices, PPE including masks and gloves availability, and any process updates such as dosage or timing changes for boosters and their relation to the primary series dose. The Team Leader included worker safety elements such as ergonomics in continuous monitoring and real-time intervention, as appropriate.
Operational and Financial Evaluation
As part of the clinic operations, records were maintained regarding supply and vaccine use, vaccine waste, personnel (LMPHW and volunteers), number of individuals coming for vaccination, and any post-vaccination adverse events. Following every event, a debrief was performed to identify what went well and any areas of concern. Feedback was gathered from workers as well as individuals who had been vaccinated and was discussed during the debrief Comments were returned to the KNA CEO and the LMPHW medical director to determine what, if any, changes were needed to the process.
Results
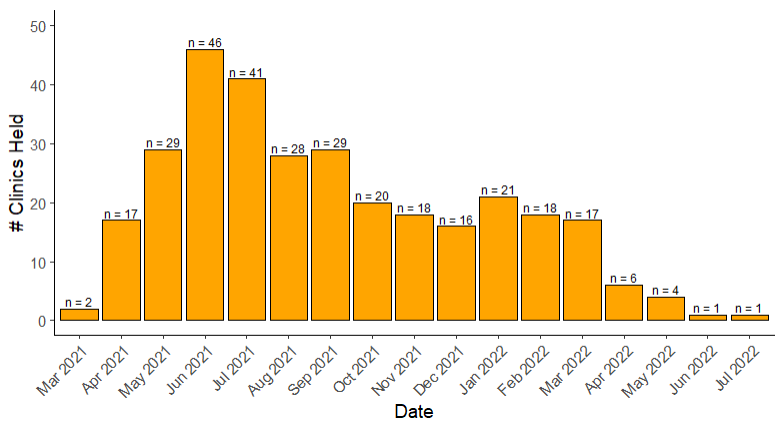
During the period spanning from March 2021 to July 2022, a comprehensive total of 8,086 COVID-19 vaccination doses were successfully administered through mobile vaccination clinics (Figure 2). Among these doses, 833 were from the Janssen vaccine, 3,557 from the Moderna vaccine, and 3,696 from the Pfizer vaccine, reflecting the broad utilization of different vaccine options in our efforts to combat the pandemic.

A noteworthy outcome of the vaccination campaign was the absence of any identified anaphylaxis events during the entire duration of the clinic’s operation. This is a significant indicator of the safety and efficacy of the administered vaccines and the careful screening and monitoring conducted during the pre-vaccination and vaccination process.
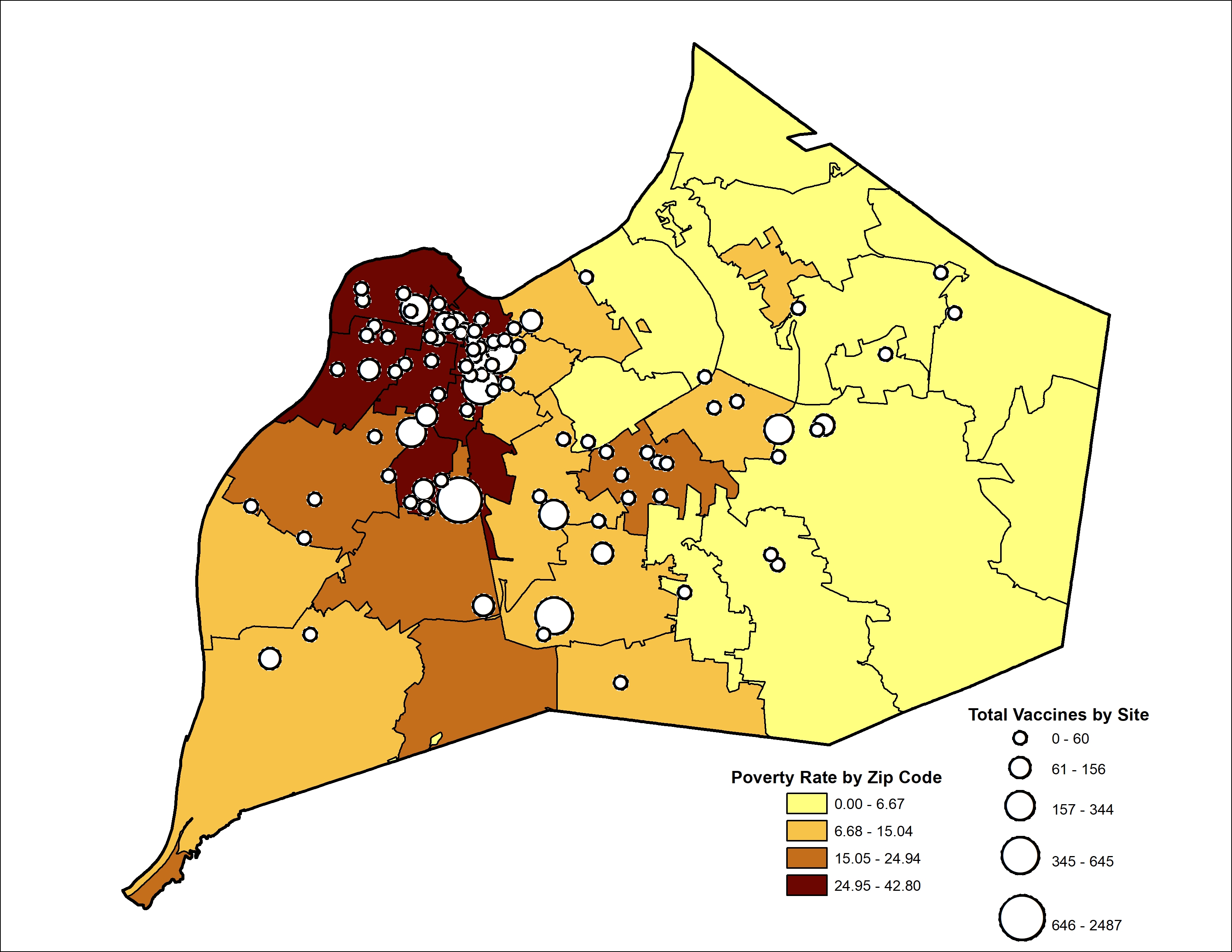
To provide a geographical context, Figure 3 presents a comprehensive visualization of the mobile vaccination sites by zip code. Additionally, this figure incorporates a map highlighting poverty rates in Louisville, Kentucky, effectively demonstrating how vaccination efforts were strategically aligned with communities most in need. The integration of these spatial data allows for a reference for the goal of providing equitable vaccine distribution and reaching vulnerable populations.

Overall, the results of this study underscore the successful execution of the mobile vaccination clinics in effectively delivering a substantial number of COVID-19 vaccine doses while maintaining a high standard of safety. Furthermore, our geographically targeted approach played a pivotal role in ensuring access to vaccinations for communities facing economic challenges. These results reaffirm the importance of flexible and community-focused vaccination strategies in combating infectious diseases and promoting health and vaccination equity.
Discussion
Challenges faced during the implementation of mobile vaccination clinics
The implementation of mobile vaccination clinics came with a set of challenges that needed to be effectively addressed. One significant challenge was the ever-evolving vaccine recommendations. Changes in booster shots, especially to accommodate any brand of vaccine, required constant adaptation and retraining of the clinic staff. Some vaccine errors regarding booster sequencing prior to guideline updates were no longer considered errors. The need for vigilance and up-to-date knowledge was critical.
Efforts to expand the mobile clinics to reach at-risk groups, such as children, posed additional challenges. Consideration for color coding and increased observation protocols become a safety modality necessary to ensure proper identification and monitoring. Moreover, catering to adult vaccine recipients, who visited the clinic less frequently, increased the potential for errors. Extra measures, like thorough record-keeping and verification processes, were implemented to minimize mistakes.
Cultural competency was crucial during LouVax-Mobile vaccination clinic operations. To provide equitable healthcare, utilization of interpreters was required to assist with communication, ensuring that accurate information was conveyed to participants. Additionally, privacy concerns needed to be addressed to respect cultural norms and preferences. An additional challenge that complicated security of vaccination clinics was distrust of law enforcement; therefore the presence of law enforcement was de-emphasized to avoid deterring participants from seeking vaccination.
Overall, challenges during the implementation of mobile vaccination clinics highlighted the need for adaptability to most current guidelines and cultural sensitivity. Future mobile clinics can successfully reach diverse populations, increase vaccination rates, and contribute to the overall goal of public health and safety by addressing these challenges effectively.
Conclusion
Mobile vaccination clinics continued to be a demonstration of the strength available within a community when partnerships are nurtured and maximized. The vaccination events showed the entire community the value and importance of engaging volunteer healthcare workers and professional associations in public health responses. Lastly, KNA and LMPHW continue to work together to ensure that items such as procedure manuals and associated tools and resources are fully developed and maintained so they can be shared with others and used as a basis for how to address ongoing public health needs in addition to future public health emergencies.
ACKNOWLEDGEMENTS
The authors thank the Kentucky Nurses Association for their ongoing leadership and provision of a competent Team Leader workforce and other volunteers supporting the efforts, employees of the Louisville Metro Public Health and Wellness and the City of Louisville for their partnership in this initiative, and for local Schools of Nursing faculty and students for their participation. In addition, the authors thank the thousands of volunteers who worked together with a united goal of protecting their community. The authors also thank the community members who came to the mobile clinics for vaccination and showed their appreciation and support for the LouVax-Mobile vaccination clinics team.
ROLE OF THE FUNDING SOURCE
There was no specific funding provided for the volunteers serving this vaccination effort. Federal funding supported costs associated with public health, and city personnel as well as equipment and supplies needed for the event, and some local funding supporting the training of clinical Team Leaders.
CONFLICT OF INTEREST
There are no conflicts of interest identified by any of the authors.