Introduction
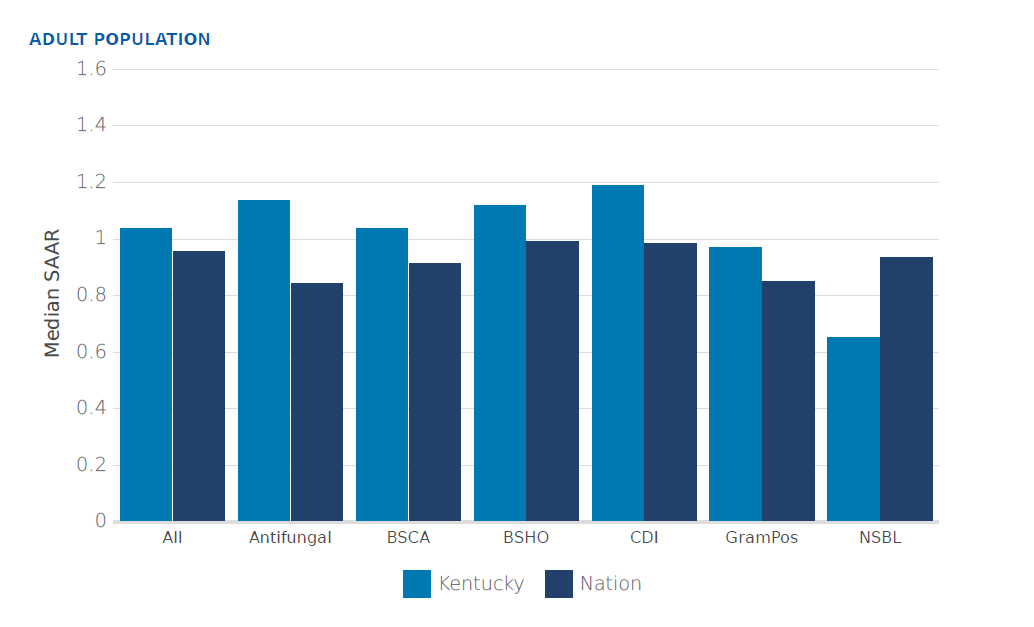
The Centers for Disease Control and Prevention (CDC) estimates that more than 2.8 million antimicrobial-resistant infections occurred in the United States in 2019, and nearly 35,000 deaths were attributed to these infections.1 Antimicrobial stewardship is recommended to reduce antimicrobial resistance by improving antimicrobial prescribing.2 Despite 98% of hospitals surveyed in Kentucky reporting that they had implemented all seven CDC antimicrobial stewardship core elements, Kentucky antimicrobial use exceeds national usage in every broad spectrum antimicrobial category (Figure 1). Furthermore, only 53% of Kentucky long-term care facilities have reported that they have implemented all antimicrobial stewardship core elements.3

Norton Healthcare (NHC) is a not-for-profit integrated health-system serving Kentucky and Southern Indiana that includes six hospitals (five in Louisville and one in Madison, Indiana) with over 1900 licensed beds and numerous outpatient clinics. NHC uses an institute structure to facilitate the multidisciplinary approach for patient care, education, and research. The Norton Infectious Diseases Institute (NIDI) is one of six current institutes at NHC. The NIDI recently partnered with the Kentucky Department for Public Health (KDPH) to develop and implement an Infection Prevention Training Center for Kentucky. Additionally, a specific focus will be to improve antimicrobial stewardship across Kentucky. To develop and guide activities in the area of antimicrobial stewardship, the Kentucky Antimicrobial Stewardship Innovation Consortium (KASIC) was launched in the summer of 2022.
In order to meet the primary goal of improving health outcomes, KASIC will seek to implement new antimicrobial stewardship programs and expand existing programs to improve antimicrobial use in the state. The aims of this manuscript are: 1) to describe the KASIC objectives, 2) to define the KASIC target audience, and 3) to describe the methods that KASIC will implement to achieve its objectives.
KASIC Objectives
The following are the primary KASIC objectives: 1) to establish an antimicrobial stewardship advisory board 2) to establish a network of antimicrobial stewardship partners, 3) to define antimicrobial stewardship program needs, 4) to improve data evaluation and visualization, 5) to develop and support implementation of interventions, 6) to evaluate the impact of interventions, and 7) to disseminate findings.
Objective 1: To establish an antimicrobial stewardship advisory board
In a recent survey of antimicrobial stewardship programs, conducted by the Infectious Diseases Society of America (IDSA), Society for Healthcare Epidemiology of America (SHEA) and Pediatric Infectious Diseases Society (PIDS), 58% of respondents reported lack of infectious diseases (ID) or antimicrobial stewardship expertise as a barrier within their program.4 To address this lack of expertise, a KASIC advisory board of experienced professions will be formed. The advisory board will represent a diverse group of academic and community institutions with long-standing and robust antimicrobial stewardship programs. The advisory board will be readily able to provide broadly applicable recommendations, stewardship resources, and mentorship to institutions with a lack of expertise.
Objective 2: To establish a network of antimicrobial stewardship partners
When addressing the public health threats associated with antimicrobial resistance, antimicrobial stewardship programs should response with a public health framework. The Kentucky healthcare system includes over 100 hospitals, including critical access hospitals, and over 300 nursing facilities.5 Therefore, to facilitate collaborative efforts and the swift delivery of communication, it is necessary to identify antimicrobial stewardship partners. These partners may include pharmacist, physician, advanced practice practitioner, infection preventionist, nursing, and executive leads at each institution with a key role in antimicrobial stewardship. Through the availability of the KASIC network, participating institutions can readily collaborate on the development and implementation of antimicrobial services such as expectant practices that can be used to facilitate evidence based anti-infective use.6 As KASIC fulfills its other objectives (described later), reporting results will be streamlined with an established network.
Objective 3: To define antimicrobial stewardship program needs
The National Healthcare Safety Network (NHSN) Antimicrobial Use (AU) Option module is supported by the CDC and facilitates risk-adjusted inter and intra-facility antimicrobial use benchmarking. Antimicrobial days of therapy per 1,000 days present serves as the primary metric reported to the AU option module. A standardized antimicrobial administration ratio (SAAR) is the primary method in which antimicrobial use is analyzed. The SAAR is calculated by dividing observed antimicrobial use by predicted antimicrobial use. Predicted antimicrobial use is generated by predictive models developed by the CDC from 2017 national data reported to NHSN.7
KASIC will work with KDPH’s Healthcare-Associated Infection/Antibiotic Resistance (HAI/AR) Prevention Program which receives NHSN AU data and has previously surveyed institutions on their antimicrobial stewardship components. The HAI/AR Prevention Program distributes inter-facility comparisons on NHSN AU option data and survey results with highlighted responses that deviated from peers. With HAI/AR data, potential opportunities for action may be identified. KASIC will serve as a resource to aid facilities in data interpretation and plans to respond. Furthermore, KASIC will provide consultations to facilitate the identification of additional antimicrobial stewardship opportunities.
Objective 4: To improve data evaluation and visualization
Antimicrobial stewardship data includes antimicrobial use data, antimicrobial resistance rates, intervention rates, recommendation rates, recommendation acceptance rates, guideline adherence, and patient outcomes. KASIC personnel will work with network members on acquiring and evaluating data. Additionally, KASIC will offer aid in visualization to assist in identifying opportunities, measuring effects, demonstrating impact, and supporting additional resource requests. Emphasis will be placed on utilizing data received from the NHSN AU option, if available.
Objective 5: To develop and support implementation of interventions
The CDC recommends seven core elements that serve as fundamental components common to all effective antimicrobial stewardship programs in hospitals and nursing homes. These core elements include leadership commitment, accountability, pharmacy or drug expertise, action, tracking, reporting, and education.2 KASIC will seek to provide examples of best practices for adaptation and mentor participating institutions in implementation.
Objective 6: To evaluate the impact of interventions
Evaluating the impact of interventions is critical for continuous process improvement. KASIC personnel will work with network institutions on identifying relevant process and outcome metrics both pre and post implementation of new antimicrobial stewardship services and practices. Furthermore, KASIC mentorship will be offered to support utilizing data to identify further opportunities and to demonstrate value to key stakeholders.
Objective 7: To disseminate findings
Other statewide stewardship collaborations have reported positive feedback from the dissemination of de-identified NHSN AU Option data.8 Additionally, peer comparison has been demonstrated to positively affect inappropriate antimicrobial utilization at the provider level.9 It is expected that this effect will also be demonstrated at an institutional level. KASIC will work with KDPH’s HAI/AR prevention program to disseminate NHSN AU Option and program survey data to the KASIC network which will facilitate institutions to benchmark and set goals. Additionally, KASIC will disseminate findings from advisory board collaborations to the KASIC network, for reference and review. Lastly, KASIC will offer guidance to participating institutions on poster, presentation, and publication creation at the local, state, and national level.
KASIC Target Audience
Select healthcare facilities with well-established antimicrobial stewardship programs will be invited to participate as members of the KASIC advisory board. Members of the advisory board will be asked to contribute examples of guidelines and protocols, develop and provide feedback on KASIC services, mentor KASIC network institutions, and aid in communication by facilitating network expansion.
The KASIC target audience will be acute care hospitals, critical access hospitals, and long-term care facilities seeking to implement or improve an antimicrobial stewardship program. It is expected that these programs will be the most likely to benefit from and readily utilize the services provided by KASIC and the advisory board.
KASIC Methods
Methodology 1: Virtual consultation (office hours)
Infectious diseases pharmacists with extensive experience in antimicrobial stewardship will serve as KASIC mentors and will designate a set time each week to be available for questions on all aspects of antimicrobial stewardship. Office hours will be conducted over video chat and be readily accessible through a set web address. Continuous feedback will be solicited to improve the experience.
Objectives met by this methodology: 3, 4, 5, 6
Methodology 2: Target educational programs
Broad educational content including didactic presentations (e.g., community-acquired pneumonia) and concise 1 – 5 minute antimicrobial stewardship and infectious diseases pearls will be developed. Specific requests for content topics will be queried from the KASIC network. Educational content will be created in multiple media types (e.g. print, video) and made readily available on a multitude of publicly accessible mediums including the KASIC website (https://kymdro.org/kasic/) and social media platforms (e.g., Twitter LinkedIn, Facebook).
Objectives met by this methodology: 5
Methodology 3: KASIC “Menu of Services”
Common antimicrobial stewardship services and content will be available on the KASIC Menu of Services (Appendix A). Multiple options are available from an array of broad categories and include:
-
Administrative
-
Microbiology
-
Education
-
Guidelines
-
Protocols and Monographs
After needs assessments have identified primary opportunities for improvement, KASIC will work with network institutions on tailoring menu items to their individual needs and mentoring network institutions on implementation. When items that are not available on the menu are created for individual institutions they will be reformatted to be generally applicable and be selectable by other institutions.
Objectives met by this methodology: 4, 5, 6
Methodology 4: Mentorship on individual projects
KASIC mentors are available to provide feedback and guidance on projects. Projects may be selected from the menu of services or proposed by the institution. Specific action items may include tailoring services to the institution, implementing, measuring, evaluating, and presenting findings.
Objectives met by this methodology: 3, 4, 5, 6, 7
Methodology 5: Mentorship on antimicrobial stewardship programs
KASIC mentors will offer coaching on how to attain and capitalize on program success. Examples of program success include decreasing broad spectrum antimicrobial utilization, increasing guideline adherence, increasing recommendation acceptance rates, and improving patient outcomes. KASIC mentors can provide effective strategies to communicate program success to improve collaboration with providers and advocate for additional support from administration.
Objectives met by this methodology: 3, 4, 5, 6, 7
Methodology 6: Establishing local best practices
With antimicrobial stewardship leaders from across the Commonwealth of Kentucky, the KASIC advisory board will seek to create local consensus on best practices. These best practices may be utilized by network institutions in support of antimicrobial stewardship recommendations or services. These best practices may serve to be more readily accepted than national guidelines as they represent local perspectives and practices through which more tangible peer pressure is experienced.
Objectives met by this methodology: 5, 7
Methodology 7: Partnering with organizations
The Kentucky Hospital Association (KHA) and KDPH’s HAI/AR Prevention Program have had on-going initiatives to improve antimicrobial use. KASIC will seek to partner with these two organizations to develop and expand the KASIC network. With the KASIC network developed, the HAI/AR Prevention Program will disseminate peer comparisons of NHSN SAAR data to antimicrobial stewardship leads and identify KASIC as an organization that can aid in data interpretation and response.
Objectives met by this methodology: 2, 3, 4, 6, 7
Discussion and Conclusions
Kentucky inpatient antimicrobial use exceeds national rates and antimicrobial stewardship implementation in Kentucky nursing homes is low.3 KASIC is a program created to facilitate antimicrobial stewardship success across Kentucky. The objectives are designed to ultimately improve patient outcomes as they relate to antimicrobial use. This will be accomplished through creation and sharing of intellectual resources provided by Kentucky antimicrobial stewardship leaders.
KASIC seeks to help its target audience overcome barriers to expansion. In a recent survey on antimicrobial stewardship programs conducted by IDSA, SHEA, and PIDS, the three most commonly cited barriers were lack of time, financial resources, and information technology.6 KASIC will be able to help institutions reduce time requirements by replacing de novo synthesis of guidelines and protocols with adaptable templates and the aid of a mentor. Additionally, to expand upon the current expectations of hospital antimicrobial stewardship programs, the Joint Commission recently announced 12 new and revised elements of performance that will go into effect on January 1, 2023.10 One of these elements supports the allocation of financial resources for staffing and information technology (IT). KASIC network institutions with newly acquired IT will have access to the collective IT experience of the KASIC network. Therefore the launch of KASIC is well opportune to aid institutions to effectively utilize the addition of new resources.
KASIC success will be primarily measured by engagement with KASIC resources. Maintained and growing engagement will signify participating institution satisfaction and utilization of resources. Specific metrics for engagement include productivity indicators such as number of projects and interactivity indicators with KASIC resources such as website views, social media views, consultations, number of office hour participants, and number of antimicrobial stewardship questions answered. Additionally, Likert scale satisfaction scores will be solicited alongside antimicrobial stewardship questions answered and highest favorable ratings will be targeted.
KASIC is not the first statewide antimicrobial stewardship effort. Other groups such as the Antimicrobial Stewardship Collaborative of South Carolina (ASC-SC) and the Duke Antimicrobial Stewardship Outreach Network (DASON) have provided exemplary models for what statewide programs can achieve.8,11,12 The Commonwealth of Kentucky will only benefit from the commencement of its own statewide effort. Moreover, because antimicrobial resistance knows no boundaries,13 the future of KASIC may be to collaborate with other statewide programs on a regional antimicrobial stewardship network.
Funding
The work is supported by the Kentucky Department for Public Health.
Conflicts of interest
All authors have no potential conflicts of interest in relation to this work to disclose.