
Background
As the SARS-CoV-2 (COVID-19) pandemic continues to unfold, community-based strategies such as mobile COVID-19 testing and vaccination have become increasingly important. Higher rates of hospitalization and death among minorities reflect higher infection rates, higher rates of underlying health conditions as well as social and economic inequities that contribute to barriers to healthcare access.1–3 Health inequities in the United States that impact minority communities have always been present, however, these inequities have become more apparent during the course of the pandemic. Underserved populations living in poverty with no insurance and limited access to primary care providers or pediatricians are more likely to have underlying medical conditions that place them at greater risk of COVID-19 related complications.1,2 An analysis by the Kaiser Family Foundation found that Black, Hispanic, and Asian individuals were more likely than White individuals to test positive for COVID-19, with Hispanics having the highest positivity rate compared to other ethnicities.3 This knowledge has become the driving force behind where the need for testing efforts is the greatest, where it could be most impactful, and where vaccination needed to occur in the community. Early detection of SARS-CoV-2 through prompt access to testing is an important COVID-19 response to slow the spread of the virus in the community,3 including the use of time-dependent interventions such as treatment with anti-viral agents.4
The need to focus on tailoring initiatives that promote health equity as a major component of the COVID-19 response prompted a collaboration between trusted leaders in the community, the Louisville Metro Public Health and Wellness Department (LMPHW), and the Kentucky Nurses Association (KNA). A specific goal that emerged from this collaboration was to provide consistent access to COVID-19 testing in an area of Louisville recognized for its poverty density and other social determinants of health. An outcome of this collaboration was conceptualization and implementation of a mobile testing clinic model where testing for COVID-19 was made available in underserved areas of the Louisville community. Specific sites for these clinics were identified by trusted community leaders. The objectives of this paper are to: 1) describe the planning approaches and strategies to support implementation of mobile COVID-19 testing clinics; 2) describe the processes by the Kentucky Nurses Association (KNA) to develop, recruit, and train the mobile COVID-19 testing teams; 3) describe implementation of mobile COVID-19 testing clinics; and 4) present real-world data to demonstrate the impact of the mobile testing clinics in the Louisville community.
Planning approaches and strategies to support implementation of mobile COVID-19 testing clinics
The mobile testing clinic was conceptualized and implemented during the first year of the COVID-19 pandemic. The approach was built upon the more than twenty years of experience with mobile and non-traditional vaccination clinics among the project planners.5,6 Initial steps involved: 1) identification of partners, 2) determining areas of community need and acceptance, 3) determining resources and methods for collaboration, and 4) developing processes that would support safe, reliable, and sustainable clinic operation. Initial planning strategies focused on immediate needs without knowledge of the growth and scope of the pandemic and what it would mean to public health and the health of the community. Planning and implementing a novel mobile testing model presented unique sets of challenges, which required the flexibility to adapt to changes in the pandemic, changes in available testing methods, needs of the populations served, and the varied skill sets of participating volunteers.
Community-based approaches used to identify and engage targeted populations for testing
The population of Louisville, KY is diverse and the census characteristics closely mirror those of the larger US population,7 in part due to the city (Louisville) and county (Jefferson County) merger, allowing for a distinct geographic area with well-defined population characteristics. There are specific areas of the Louisville metropolitan area that are recognized as underserved and where significant numbers of the population experience barriers to healthcare access and other social services. Further, the health outcomes impact of COVID-19 were more profound in specific geographic areas of Louisville, including those with an increased poverty density.8 These areas were of particular interest to local public health, for example, homeless shelters where asymptomatic carriage could represent a significant impact on transmission. The LMPHW used existing relationships to identify community partners and leaders in many of these underserved areas. This facilitated a process where community leaders played an active role in the development of a testing approach. Local community leaders worked with LMPHW to gain knowledge and build trust as a means of shifting the locus of control to the community. In collaboration with community leaders, content experts from the nursing, medical, and public health communities participated in listening sessions, town hall meetings, and open forum discussions to facilitate knowledge exchange and trust-building. These conversations led community leaders to identify locations within recognized at-risk communities that could be used as a COVID-19 testing sites and where there was local interest and acceptance of testing. Community members were essential for establishing the testing strategy through a community-based process, as opposed to a community-placed process in which testing locations were determined by those outside the community5 This process was used by LMPHW to develop the iterative testing site list, site contacts, and preferred hours/days of testing clinic operation and where KNA would plan and implement testing clinics.
Strategies used to engage the targeted populations for testing
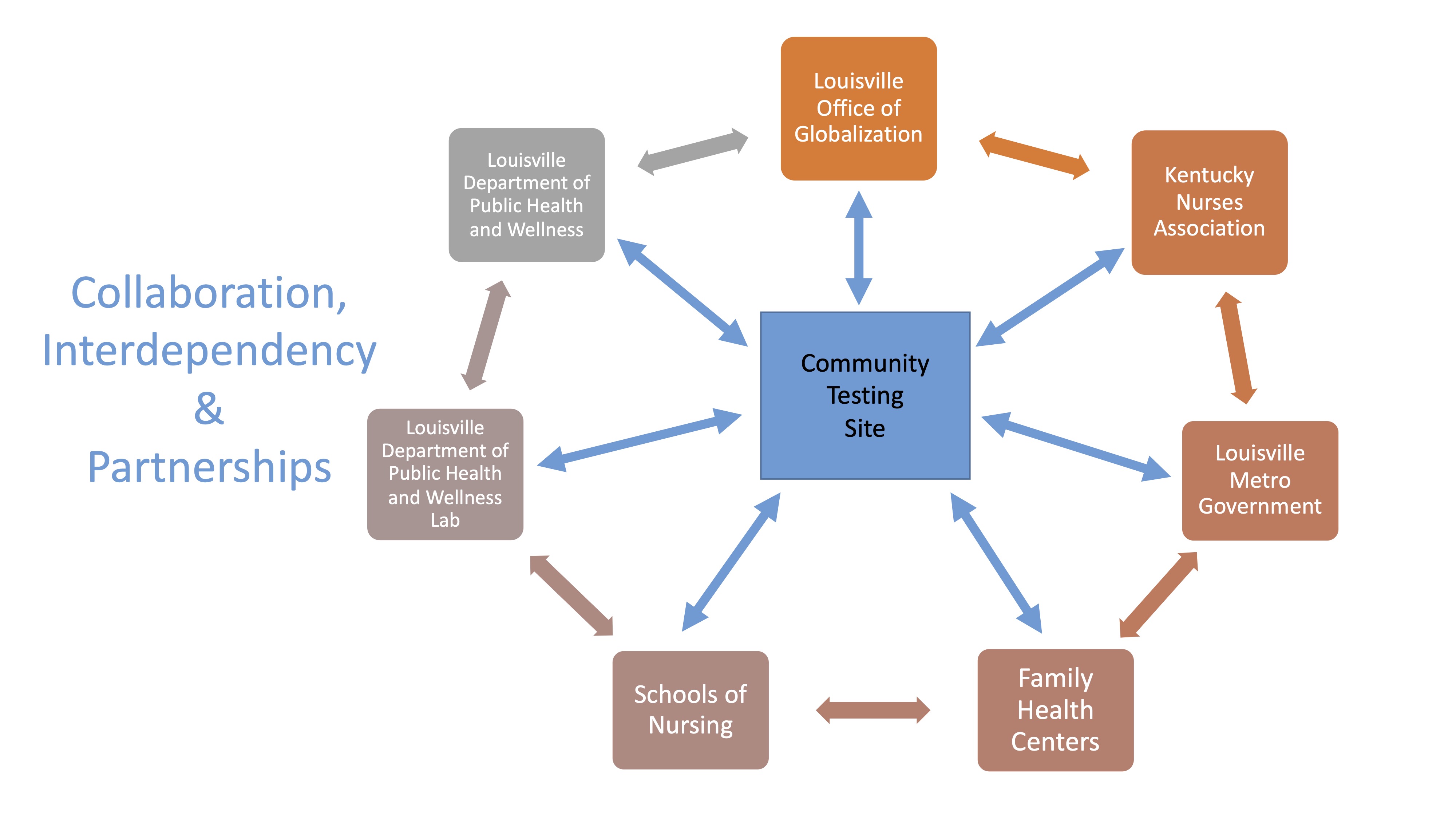
Community-based interactions produced two major points: 1) testing needed to follow the elements of community-based approaches, and 2) the workforce involved in addressing COVID-19 testing needed to reflect the populations served. Sites needed to be determined by individuals within the targeted communities and structured with the needs of those community members as the driving force. Resource needs varied across communities (e.g., some communities needed translators, some communities required security, community response would vary in size). Attention to workforce diversity included race, ethnicity, language, culture, and religion as well as the professional competence of those workers. The ability to provide this ‘goodness of fit’ brought KNA to the forefront as a major and pivotal community partner. Figure 1 depicts the depths of collaboration, interdependency, and partnerships vital to this endeavor.

Development of mobile testing clinic teams
Using outcomes from the community-based interactions, a primary goal emerged focused on providing access to COVID-19 testing in some of the most underserved areas in Louisville, Kentucky. Planning for testing involved determining the ideal skill sets and structure needed to build competent and sustainable mobile testing teams. Skills sets were role-based with some including a scope of work necessitating professional clinical licensure while others required administrative and clerical expertise. All roles involved knowledge and application of basic elements of infection prevention and control. Intangible skills included an ability to work with a multidisciplinary team and multicultural population as well as have emotional intelligence and the ability to adapt. These skills were needed as part of pandemic response during times of stress, fatigue, and the ever-present unknown. This information was used to develop a training process, recruit a diverse group of individuals in an attempt to mirror the local community, set expectations, and conceptualize competencies and training.
KNA took the lead in planning, coordinating, and implementing the day-to-day operation of testing clinics. KNA developed Standard Operating Procedures (SOP) for all elements of the mobile testing approach. This SOP is included as a supplementary component to this manuscript.
Clinic site information was provided by LMPHW and a site visit was performed by the KNA Chief Executive Officer (CEO) in order to assess workflow, local site contact, and safety. Once a site had been visited and evaluated, it was added to the clinic site list, maintained by KNA. The KNA CEO worked with a local APRN with extensive experience in infectious diseases and public health, designating them to be the project leader. The project leader developed a standardized workflow and identified components for orientation and training for clinic volunteers. These elements became the Standard Operating Procedure (SOP) and continued to be updated and expanded throughout the implementation of mobile testing clinics. As a pilot process, five clinics were held in the first two months of the initiative. These pilot clinics demonstrated the importance of having a team led by a nurse capable of patient assessment, patient care relevant to performance of testing, infection prevention and control, team leadership, training, oversight, and communication. Additional clinic personnel were needed to: 1) welcome and register individuals coming for testing, 2) perform the nasal swab/nasopharyngeal swab, 3) perform the rapid antigen test, and 4) document all clinic activities and communications. Lessons learned from this pilot phase laid the groundwork for an extensive, long-term project, capable of adapting to the needs of the community. The first step involved identification of a group of experienced Registered Nurses (RN) and Advanced Practice Registered Nurses (APRN) willing to serve as team leaders. These Team Leaders (TLs) would be responsible for managing and facilitating the testing clinics. The KNA CEO recruited active KNA members with an interest in, and available time to help with, COVID-19 control efforts. An electronic sign-up process (SignUpGeniusTM) was used to enable volunteer sign-ups, volunteer engagement, and site staff planning. Leadership, clinical acumen, flexibility, excellent communications skills and a community-focus were attributes deemed as important for TLs. As the effort evolved and activity increased, new TLs joined from the ranks of nursing volunteers at mobile testing and other KNA events. The KNA office maintained records of TL orientation, training, and preceptor-mediated mission experiences. Each TL candidate was required to complete two testing mobile clinics as an observer and one testing mobile clinic independently, precepted by an experienced TL. Using funds provided by the LMPHW, TLs were provided a nominal hourly stipend and mileage reimbursement, and the role continued on a voluntary basis. Administrative support was provided by KNA in order to maintain recordkeeping of events, personnel, supplies, and summary reports. Logistics support was also provided by KNA. This involved procurement of testing supplies, performance of controls of the antigen tests to be used at that clinic, delivery of all testing items to the clinic sites, assistance with clinic set-up, gathering supplies at the end of each clinic, cleaning and disinfection of items, and restocking in preparation for the next clinic. Logistics support also provided help to TLs with orientation and education for any clinic personnel prior to implementation of each testing clinic. Prior to any clinic, a checklist was prepared including: 1) information about the site, 2) the site contact, 3) name of the TL, 4) additional volunteers able to serve in administrative, specimen collection, and test performance roles, 5) number of anticipated tests to be performed, 6) supplies necessary for the clinic, 7) documentation forms, and 8) job aides outlining the roles and responsibilities for each member of the clinic team. This information was included with the supplies delivered to the site and reviewed with the TL by KNA logistics support.
Recruitment and training of the mobile testing teams
Initial recruitment was done through the KNA network. During the early phases of the pandemic, KNA members had been involved in current pandemic response efforts, prior public health response events, and were familiar with a number of community and public health leaders engaged in response activities. This helped gather what would become the mobile testing core at KNA and led to growth building upon relationships and peer groups of that initial core. An example of that growth included expansion to include faculty and students from local schools of nursing.
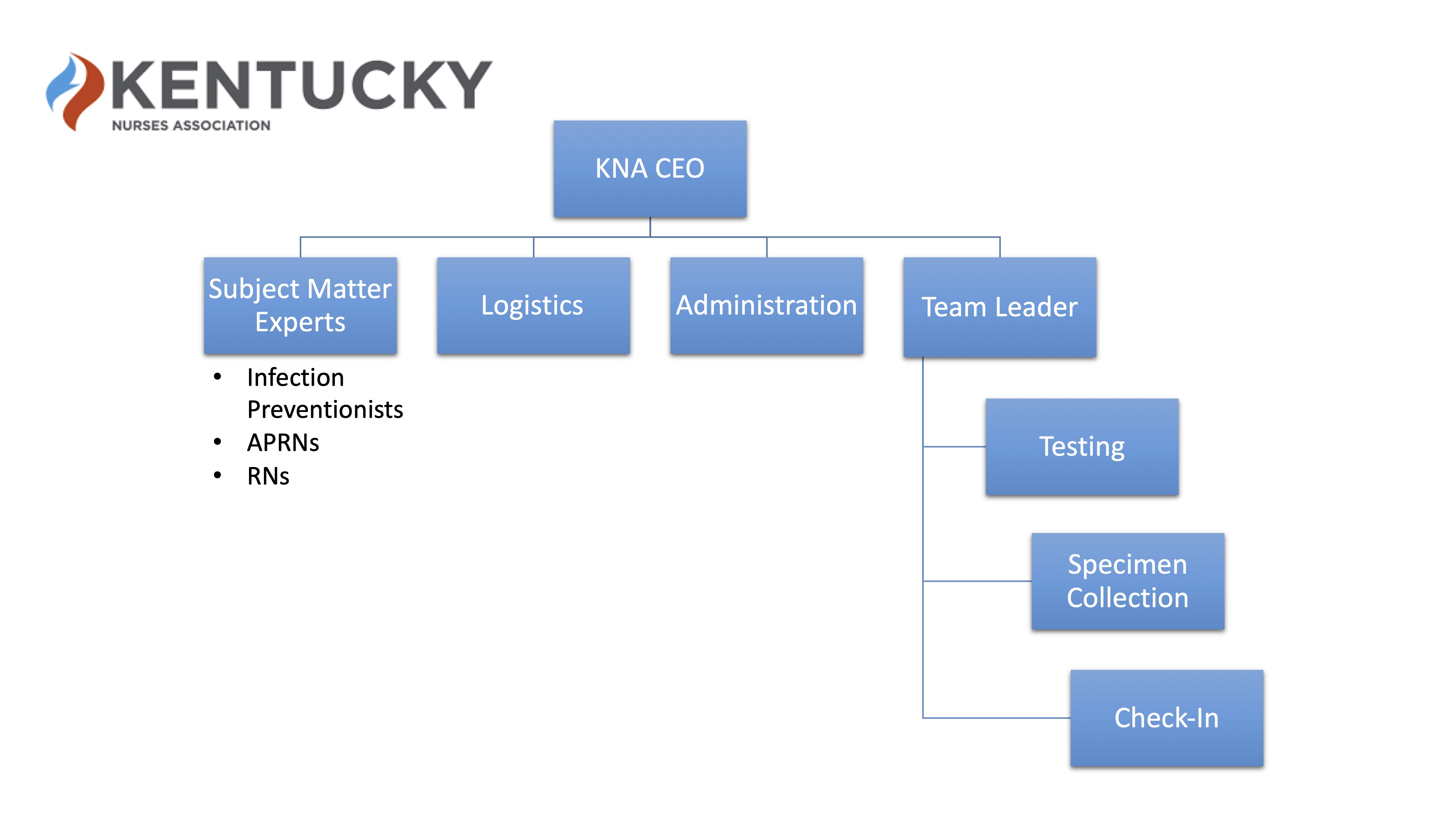
Figure 2 depicts the mobile testing team personnel. Leadership for the teams was managed by the KNA CEO. This included oversight of the program, reporting back to LMPHW, administrative responsibilities including report development, and supply and logistics. At the testing site, personnel included the TL, registration, specimen collection, and specimen testing. Site maintenance such as disinfecting surfaces before and after events and gathering of waste was part of the entire team’s responsibility. A complete description of roles and responsibilities for each member of the team are included in the SOP provided as supplementary material to this manuscript.

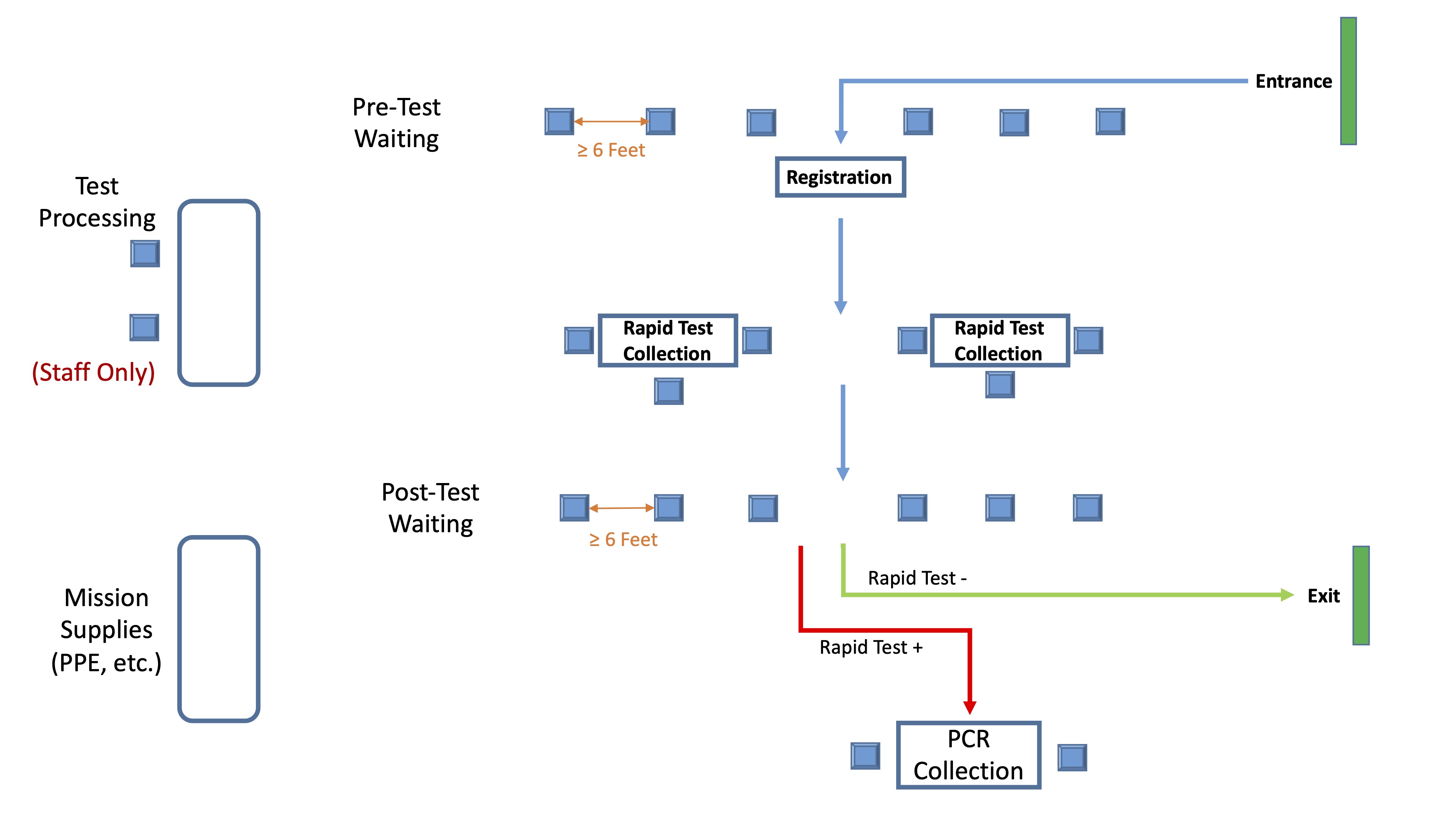
Individual training and orientation to the role was done prior to the beginning of all clinics. The workflow of the clinic was used in the training process to show how individuals coming to the clinic for testing would be routed through the process and where key activities would occur (e.g., registration, specimen collection, specimen testing). The typical clinic setup and workflow are shown in Figure 3. Responsibilities requiring patient contact (e.g., collection of specimen, donning and doffing of personal protective equipment [PPE]) and performance of testing (e.g., antigen test) also included specific competence verification. Examples of these competencies are also included in the supplementary materials. Safety was a critical component of training for all individuals. This included infection prevention and control activities such as use of PPE, hand hygiene, environmental disinfection, masking of everyone at the testing sites, and use of social distancing practices. Routine safety practices also included elements specific to COVID-19 such as testing of team members to identify asymptomatic infection and assessing presence of signs and symptoms associated with COVID-19 prior to the mobile testing clinic.

Implementation of mobile testing clinics
Details regarding the implementation and operation of mobile testing clinics are outlined in greater depth in the supplementary materials. Implementation of a mobile testing site consisted of two phases, the clinic and post-clinic phase.
Clinic Phase
The clinic phase involved set-up, orientation of clinic personnel, monitoring of clinic flow, and documentation. A standardized set up was used for the clinics that enabled an organized workflow, as depicted in Figure 3. Prior to the beginning of a clinic day, all volunteers were tested for COVID-19 using rapid antigen testing. Anyone with a positive test was immediately excused and local public health was notified in accordance with public health testing and reporting requirements. Testing personnel donned PPE relevant to their roles and responsibilities (e.g., gowns, gloves, respirators and face shields worn by personnel at the specimen collection and specimen testing areas; masks or respirators worn by those at the registration area). Orientation included a review of PPE selection, donning, doffing, and use; performance of nasal swab/nasopharyngeal swab; performance of the laboratory test using the rapid antigen test available at that clinic; patient education; documentation; infection prevention and control measures; and emergency response. The entire testing area was disinfected using disinfectant wipes (EPA List N) as a first step in the clinic setup and the last step when closing the clinic session. Alcohol-based hand rub and tissue were available throughout the clinic area. Individuals reporting to the site for testing were seen at a registration area to provide name and demographic information needed for public health reporting in the event their COVID-19 test was positive. Individuals then moved to a specimen collection area where they could be seated while the specimen collection process was done. Once their nasal or nasopharyngeal swab was obtained, they were directed to a waiting area where they would stay until their test results were available. During operation of the pilot clinics, rapid antigen tests were not yet available. Nasopharyngeal swabs (NP) using polymerase chain reaction (PCR) testing procedures were used. The swabs were obtained, labeled with the individual’s information, and taken to the local health department laboratory for testing. Individuals were notified of test results using health department procedures. This became the process used whenever a PCR test was sent to LMPHW from any of the testing clinic sites.
In August 2020, the BinaxNOW™ rapid antigen tests became available and antigen testing quickly became the primary testing process used. Following directives from LMPHW, rapid antigen tests were done with a reflex to PCR in the event the antigen test was positive. A variety of antigen tests were subsequently used, depending largely upon supply availability. This required continuing training and competence verification. At the specimen collection area, nasal swab was performed and immediately handed off to volunteers at the testing area. There, the antigen card was labelled with the individual’s name and time the test card was activated with reagent, and the testing process was performed. Timers were used to ensure a consistent process and adherence to the test instructions for use. Individuals were notified of negative results at the site by the TL or site contact. Positive test results were communicated directly to the TL, who then notified the individual, or worked with the site contact to notify them. Those individuals were directed to return to the specimen collection area where an NP swab was collected for PCR. Those samples were taken to the LMPHW laboratory for processing. PCR test results were communicated to the individual through LMPHW procedures, usually the following day. Individuals with presumptively positive COVID-19 tests (e.g., positive antigen test but waiting for PCR confirmation) were isolated following pre-determined protocols outlined between LMPHW and the community site. As COVID-19 vaccines became available, these mobile testing sites also became sites for vaccine administration to individuals with negative tests, if desired.
Post-Clinic Phase
At the end of the clinic, disposable items were bagged for disposal. Environmental disinfection was performed and items repacked for KNA logistics to gather, reprocess, and repack for the next clinic. The TL completed a clinic summary document noting number of individuals tested, positive and negative test results, and any unusual situations that may have occurred during the clinic operation (e.g., invalid tests). Volunteers were gathered for a short debrief session where the TL led a discussion seeking to identify opportunities for improvement. This feedback was also brought back to the KNA CEO and included as an agenda item for bi-weekly TL calls. This process supported the iterative approach used to identify opportunities for improvement as well as error identification, ‘near miss’ situations (e.g., identification of expired reagents and test cards before use), and process deviation.
Impact on the Louisville Community
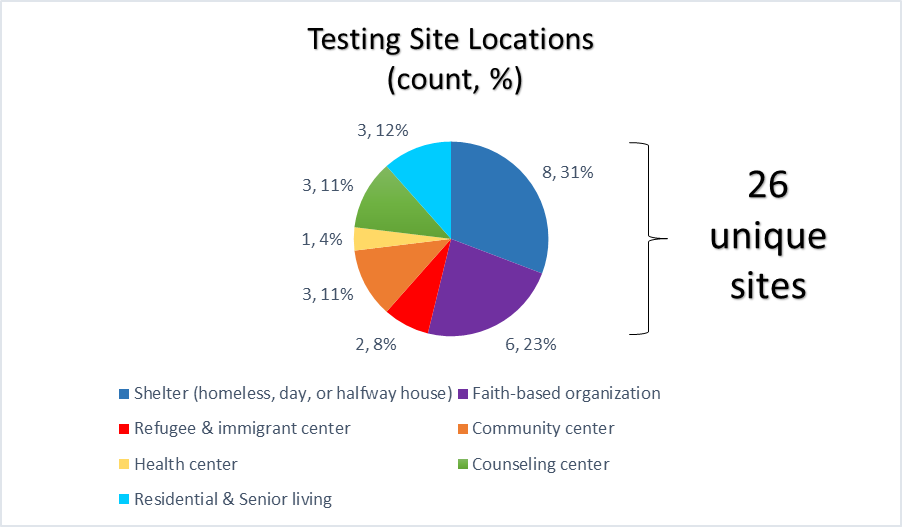
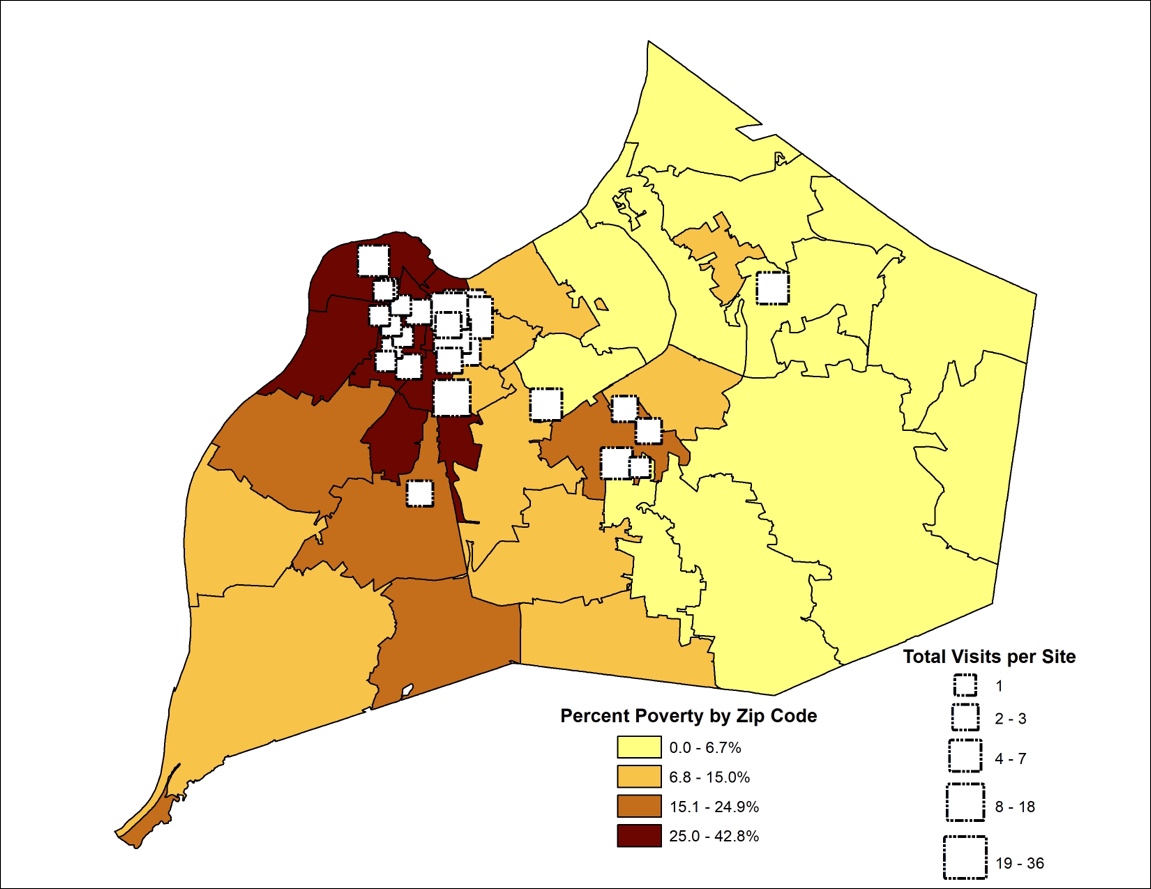
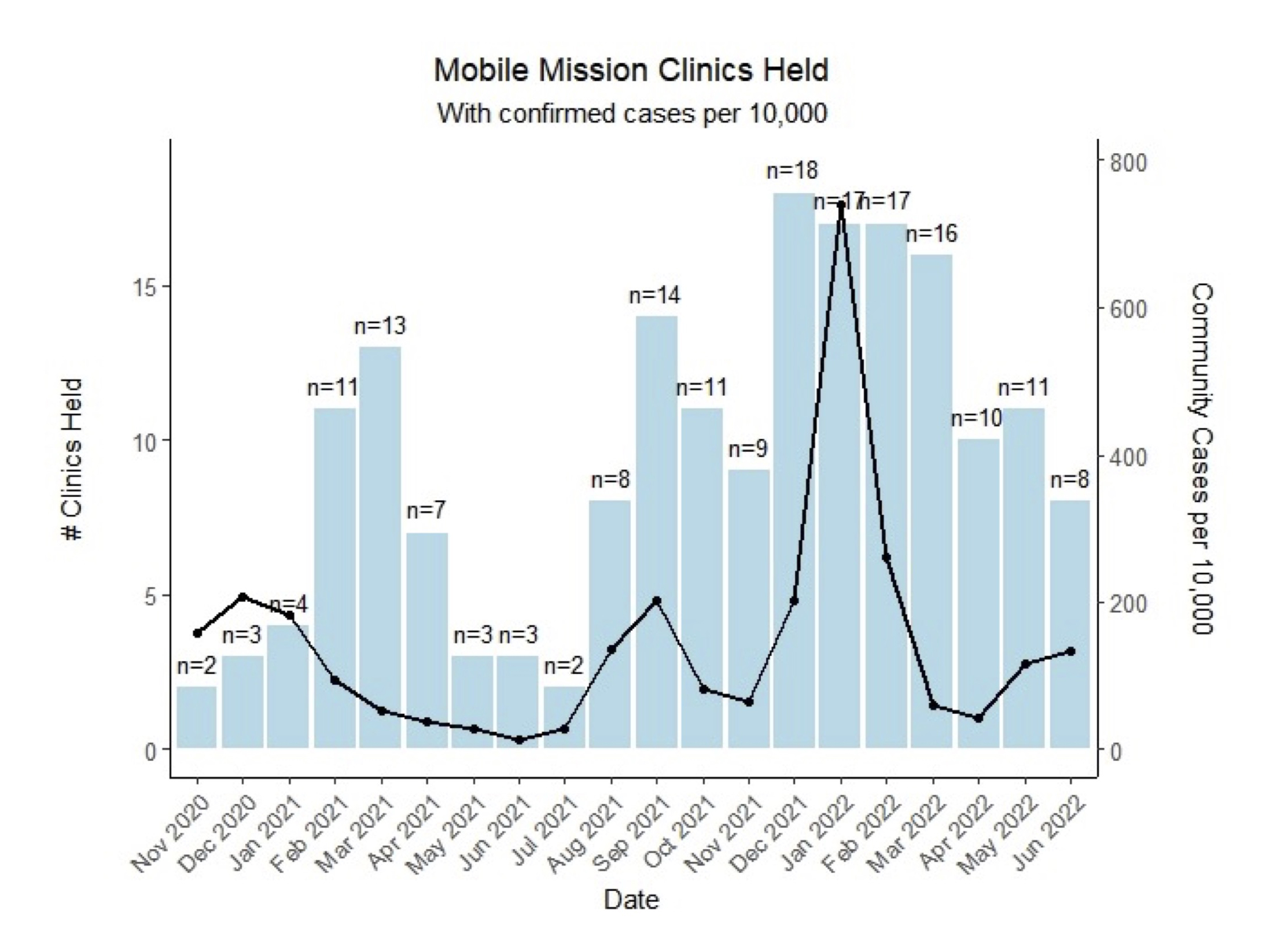
The first mobile testing clinic was held on November 11, 2020. From that date through June 30, 2022, 187 mobile testing clinics were held at 26 unique sites. Figure 4 depicts the type of setting for each testing site. Figure 5 depicts a choropleth map of poverty within each Louisville/Jefferson County zip code taken from the US Census Bureau9 with graduated symbols overlaid indicating the locations of the clinic sites, with symbol size corresponding to the number of mobile testing clinics held at that site. Figure 6 uses the same choropleth map but the graduated symbols depict the total number of tests performed at each clinic site instead. At those 187 clinics, 9337 tests were performed and 68 of those clinics occurred during a recognized outbreak among individuals either staying at the site (e.g., shelter) or within the population frequenting the community site. Figure 7 depicts the clinic calendar and outlines the relationship between mobile testing clinics held and COVID-19 cases in the Louisville community between November 2020 through June 2022 taken from the CDC.10 As COVID-19 cases increased in the community, a direct response to this increase was that additional testing clinics were held. This is a clear demonstration of how mobile testing sites worked with the community and continued to respond to their immediate needs. Each clinic was in operation for 1 to 5.5 hours, corresponding to 4,106 volunteer-hours in total. Clinic operation depended upon the number of individuals anticipated to request testing at the site, with a range of 3 to 259 individuals tested.




Clinic Team Characteristics
A total of 14 TLs were trained by the project leader; 7 (50%) TLs were registered nurses and 7 (50%) were advanced practice registered nurses. Twelve TLs were female and two TLs were male. Seven TLs were white, six TLs were black or African-American, and one was Asian. A total of 750 additional volunteers were part of the staffing for those clinics, which included registered nurses, nursing students with a faculty member, volunteer healthcare workers including medical assistants, or researchers.
DISCUSSION
The SARS-CoV-2 pandemic made evident the need for a strategy that accounted for the depths of health inequities and ensured equitable responses. Despite the knowledge of existing public health inequities in Louisville and the funding and support for pandemic response, we found that the existing, funded infrastructure was insufficient for reaching vulnerable individuals and communities. This testing approach used available public health resources and was driven by a volunteer workforce to provide testing in areas of high need and limited pre-existing resources.
The community-based model provided community members the ability to voice where public health resources should be directed. The collaboration allowed community leaders to determine sites without the concern for logistics or financial risk. To our knowledge, we were the only organized testing approach using a community-based model to provide this service in Louisville. Further, there are limited reports of this type of a volunteer-driven approach in other areas of the country.
KNA’s leadership in this initiative was paramount to its success. The staffing of clinics by nurses enabled a credible approach that leveraged the community’s trust in nurses. This builds upon the long-standing findings with the public identifying nurses as the most trusted profession.11 Additionally, this credibility allowed KNA to provide education to the community regarding infection prevention and control, the importance of testing, and ultimately the importance of vaccination. These conversations set the stage for discussions involving vaccine hesitance and vaccine confidence with community members.
The approach outlined in this manuscript and SOP has shown to be sustainable. Despite the availability of at-home tests, mobile testing clinics continue to be held in the Louisville community to address vulnerable population needs (e.g., homeless without a mailing address). Ongoing training engages new TLs and volunteers as well as sharpens competencies of existing TLs and volunteers. The basis for this approach has also been used to develop mobile vaccination clinics that are also volunteer-driven. This model is also being used to develop similar approaches in other areas of the Kentucky commonwealth.
In conclusion, we developed a unique approach that has proven to be successful in engaging community interest and serving vulnerable populations. This model, developed during a time of crisis, can continue to guide a new public health paradigm in a post-pandemic time.
ACKNOWLEDGEMENTS
The authors would like to thank the following individuals for their assistance with the Mobile Missions-Testing clinics and the logistical support required for the events: Joseph Carrico, Sherry Chandler, Kimberly Becker, participating Louisville community leaders, and the Kentucky Nurses Association Team Leaders and volunteers.
ROLE OF THE FUNDING SOURCE
Funding was provided to the Kentucky Nurses Association by Louisville Metro Department of Public Health and Wellness to purchase testing supplies, some support for logistics, and some stipends and mileage for Team Leaders. Louisville Metro Department of Public Health and Wellness also provided test kits, some testing supplies, and performance of laboratory PCR testing for positive COVID-19 antigen tests. No funding was provided for development of this manuscript.