

Introduction
The insidious rise of antimicrobial resistance has become one of the most urgent threats to modern global health.1 Although the threat of multi-drug resistant infections has been present for decades, a recent increase in such infections has been observed in the United States, likely secondary to lapses in antimicrobial stewardship (AMS) through the COVID-19 pandemic.2 This collateral damage was unfortunately foreseen by experts, and emphasizes how vital it is to improve AMS practices moving forward.3
The southern region of the United States has consistently utilized more antimicrobials than other areas of the nation, with the most recent data demonstrating that West Virginia, Alabama, Louisiana, Kentucky and Arkansas compose the top five states for outpatient antibiotic use per capita.4 It is imperative to emphasize the importance of AMS and capitalize on existing opportunities. Our aim is to describe the state of AMS in Kentucky, as the issues identified may resonate with other experts, particularly those within the South.
Methods
The Kentucky Antimicrobial Stewardship Innovation Consortium (KASIC) was formed to address antibiotic use throughout the Commonwealth of Kentucky. The KASIC advisory board is composed of 26 pharmacist experts in infectious diseases (ID) and AMS, representing 13 healthcare institutions and 2 colleges of pharmacy within Kentucky.5 An open call to participate in manuscript development was extended to the advisory board. The authors then performed a Strengths, Weaknesses, Opportunities, Threats (SWOT) analysis to describe the state of AMS in the Commonwealth of Kentucky based on their own experiences.
Results
Antimicrobial Stewardship Strengths in Kentucky
A focus on basic AMS practices has already been emphasized in many Kentucky healthcare institutions. Ninety-two percent of Kentucky hospitals report compliance with the CDC’s 7 Core Elements of Antimicrobial Stewardship, with a notable core element including establishment of an AMS program. This compliance rate is similar to the national rate of 91%. Additionally, as of June 2021, 39% of Kentucky hospitals had reported at least one month of data to the National Healthcare Safety Network (NHSN), which is a higher reporting rate than 80.7% of states and territories.4 There also appears to be some modest decrease in outpatient prescriptions in Kentucky over time (Figure 1 & 2).6–9


In addition to having metrics to describe AMS, new expertise in ID continues to grow in Kentucky. The state is home to both ID physician fellowship and specialized clinical pharmacy training programs and has more board-certified ID pharmacists than other states with similar antibiotic prescribing patterns, suggesting AMS expertise may be more accessible.10 Additionally, AMS has become an integral part of healthcare education. A more comprehensive curriculum including didactic learning, rotational experiences, and post-graduate training emphasizes the importance of AMS early on and throughout training, even outside of ID training programs. Empowering learners across all disciplines and specialties with AMS knowledge is likely to pay dividends for decades to come.
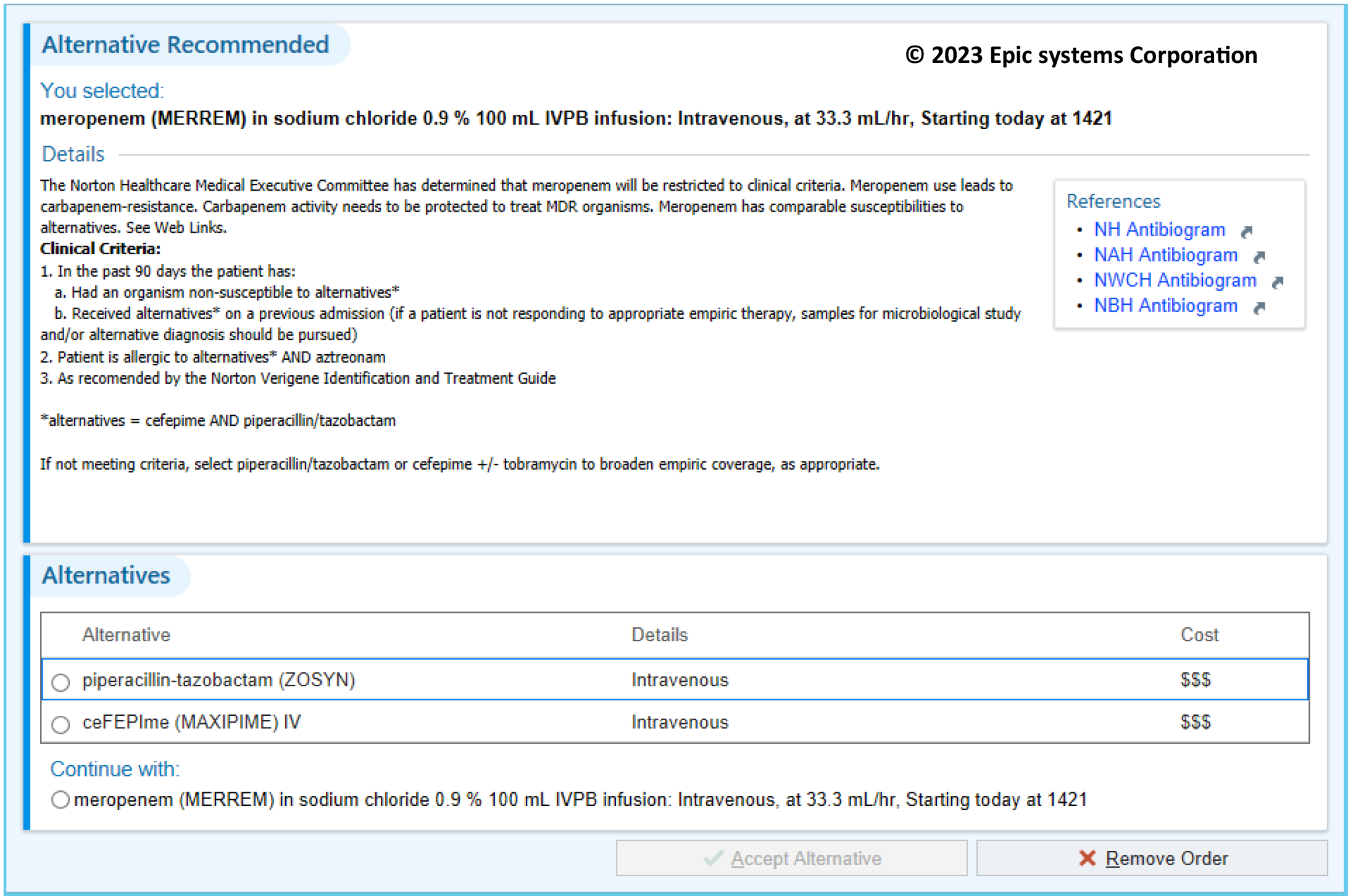
Within the Commonwealth of Kentucky, there have been several institution-specific innovations to expand the scope of existing AMS experts in the acute care hospital setting. One such example is the development of an opt-out AMS approach, which allows antimicrobial stewardship staff to update medication orders without direct authorization from a prescriber after a set period of time. This system operates under the assumption that prescribers wish to perform antimicrobial optimization when recommended by a stewardship expert, instead of continuing current antibiotics without optimization.11 Additionally, clinical pharmacists have been leveraged to decrease time to effective antibiotic therapy in patients with bacteremia.12 AMS pharmacists have also enlisted the aid of pharmacy residents and non-ID specialized staff. These AMS extenders can be trained and empowered to perform regular AMS duties such as reviewing therapeutic restrictions. This practice both emphasizes the importance of performing AMS as part of early career education and empowers individuals outside of ID experts to participate in the shared responsibility of AMS. Finally, clinical decision support technology has been implemented in the electronic medical record (EMR) to guide prescribing and decrease use of unnecessary broad spectrum agents (Figure 3). These types of AMS interventions may be helpful in decreasing inappropriate prescribing at the point of order entry and decrease the downstream workload of staff performing prospective audit and feedback. AMS experts’ dissemination of successful interventions both at a state-level and beyond may aid other institutions in implementing similar programs.

Antimicrobial Stewardship Weaknesses in Kentucky
Kentucky’s antibiotic use makes it an outlier within the United States as a whole. The state’s prescribing rate has consistently been among the top five highest within the United States in the last five years, as measured through outpatient antibiotic prescriptions per 1000 residents (Figure 1).6–8 Additionally, Kentucky’s state level standardized antibiotic administration ratio (SAAR) for inpatient antibiotic administration ranked the sixth highest of the reporting states in 2021 at 1.103 (CI 0.965 – 1.131).13 Together, these data demonstrate a need for continued AMS efforts to optimize antimicrobial use across inpatient and outpatient settings.
The overall antibiotic use data is high relative to the rest of the nation, but Kentucky’s inpatient prescribing data is incomplete. With <50% of Kentucky facilities reporting their antimicrobial use, the accuracy of benchmark statistics is likely skewed.4 In facilities which have not reported, it is likely that antimicrobial use data may not be readily available. Though staff at these facilities may be aware that state-level data suggests antimicrobial overuse, advocating for practice change may be difficult without local evidence.
In addition to overall high prescribing rates, the rates of fluoroquinolone prescribing in Kentucky are among the highest in the United States.9 Fluoroquinolones are particularly problematic given that they pose a high risk for both the development of antimicrobial resistance and Clostridioides difficile infection (CDI).14–16 Though fluoroquinolone prescribing rates have decreased as of 2021, Kentucky’s use rate was nearly 50% higher than the national average (67 prescriptions per 1000 population vs 45 prescriptions per 1000 population).9
Kentucky also suffers from a lack of ID physician expertise. Nearly 90% of Kentucky counties do not have an infectious diseases physician, with rural areas appearing to be particularly underserved.17 This lack of ID physician access could contribute to both suboptimal decision-making in the care of complicated patient cases as well as less robust leadership of local AMS programs. Finally, Kentucky has traditionally lacked a formalized state-level AMS network. Though AMS experts may connect organically or through other professional organizations, there has not been an organized forum to exchange ideas on how to improve AMS in Kentucky.
Antimicrobial Stewardship Opportunities in Kentucky
Fortunately, opportunities to improve AMS in Kentucky are plentiful but do require action. One such opportunity is increasing transparency surrounding antimicrobial use, both within individual healthcare institutions and the state as a whole. This would provide further insight into what AMS opportunities exist. Without locally validated data or benchmarks versus peer healthcare institutions, it is difficult to make the case that antimicrobial use needs to be improved and thus the status quo is likely to be upheld. If prescribers are able to review data suggesting their practice is an outlier, they may be more motivated to implement practice change.
Though a mentioned weakness was the longstanding lack of a formalized AMS network, Kentucky has now established and is expanding its state-level antimicrobial stewardship initiative.5 KASIC provides access to AMS expertise and mentorship for facilities that are working to further develop their AMS services. Its establishment was supported by the Kentucky Department for Public Health, which demonstrates increased emphasis on AMS by local and national entities. This type of investment illustrates concerted efforts to improve the quality of AMS services provided. Other states have been successful in establishing state-level AMS collaborations, creating resources based on local data and championing AMS.18
With the establishment of a formal AMS network, the barrier to connection and collaboration is lower. The increased utilization of technology, including social media and teleconferencing, has made it easier than ever to network with AMS experts and support the exchange of ideas. Given fewer barriers to access, services like telestewardship are more attainable than in the past. Increasing accessibility can facilitate statewide antimicrobial education and streamline exchange of improvement ideas.
Although healthcare stakeholders have started to focus on AMS quality improvement, there is substantial opportunity to exert additional influence aimed at improving AMS quality across various healthcare settings. For instance, the Centers for Medicare & Medicaid Services has announced changes to hospital conditions of participation which includes addition of the Antibiotic Use and Antibiotic Resistance (AUR) surveillance measure. This will require participating hospitals to actively engage with NHSN by submitting to AUR data starting in 2024.19 Raising standards for data transparency and quality of stewardship by accrediting bodies, quality assurance organizations, and payer stakeholders will financially motivate healthcare leaders to prioritize AMS and dedicate the necessary resources to improve quality of care.
Finally, though pharmacists and physicians most often serve as AMS leaders, there is a growing call for an integrated, multi-disciplinary approach to AMS. Other disciplines including, but not limited to, bedside nurses, infection prevention staff, nurse practitioners, physician assistants, microbiology professionals, veterinarians and dentists are all being called into the fold of AMS.20,21 Each of these disciplines bring a unique skill set that will likely increase the scope and quality of overall AMS services.
Antimicrobial Stewardship Threats in Kentucky
Kentucky AMS experts agree that a lack of prescriber education surrounding antibiotic optimization is a major threat to improving antibiotic use, and ultimately patient outcomes. Areas for improved provider education include antimicrobial spectrum, current clinical practice guidelines, advances in clinical microbiology and which anti-infectives pose the highest risk for the development of resistance, CDI, or adverse drug events.
As an added layer of challenge, the health practitioner training model relies on apprenticeship-style learning, meaning mentors teach and dictate trainee practices. This poses unique challenges when it comes to establishing practice change relative to other industries. If a mentor is not utilizing the most current evidence-based practice, a trainee has several barriers to overcome in order to enact change. They must first self-educate on a topic, recognize the gap in best practice and their mentor’s practice, then either advocate successfully against the more experienced mentor or wait, potentially for years, until they have completed their own training to begin enacting their proposed practice change. This teaching model, which exists across healthcare disciplines, makes it vitally important for established practitioners who teach learners to self-educate on AMS so they may pass on best practices.
One reason AMS may not be a priority for healthcare practitioners’ self-driven continuing education may be the mistaken belief that antimicrobial resistance is inevitable and/or irreversible, and therefore, AMS is futile. Additionally, prescribers may be unaware that failure to de-escalate antibiotics is associated with inferior clinical outcomes.22,23 If AMS is not viewed as a worthwhile knowledge base, it is unlikely to be studied or taught. Furthermore, the misunderstanding is likely to slow uptake of good AMS practices.
Though the previously mentioned threats primarily relate to a lack of education or awareness, another major issue is ensuring dedicated staff and time are reserved for AMS. Competing priorities, such as pandemic response, may make it exceptionally difficult to provide consistent or robust AMS. Support from institutional leaders and administrators would not only improve AMS efforts but could be a key factor in preventing burnout amongst AMS staff.24,25
Other threats are related to the baseline health status of Kentuckians as a whole. Kentucky is plagued by high rates of smoking, chronic obstructive pulmonary disease, overdose related deaths and new human immunodeficiency virus (HIV) infections.26–29 Kentucky also has a unique threat as it relates to people who inject drugs and the ID complications that can be linked to this patient population. A national survey was conducted by the CDC and found that 54 Kentucky counties are at high risk for rapid spread of HIV and high rates of hepatitis C.30 Patients are also likely to be medically underserved, particularly in the rural Appalachian area of the state. Eastern Kentucky, which falls into the Appalachian region, also has higher antimicrobial use per capita.31,32 Poor baseline health status coupled with a lack of access to care likely puts Kentuckians at risk for a multitude of poor health outcomes, including those related to suboptimal antibiotic use.
Finally, it may be possible that there are prevailing or particularly strong cultural beliefs held surrounding antibiotics throughout Kentucky and the South as a whole. It may be that prescribers, patients or both have a skewed risk versus benefit assessment that contributes to relatively high antibiotic prescribing. However, if this phenomenon is a factor, it would be difficult to measure objectively and as outlined throughout, there are many objectively-measured and documented AMS issues to address.
Conclusion
The disparity of antibiotic prescribing and AMS success within Kentucky and the United States’ southern region is a cause for concern. To improve this disparity, a concerted effort from local stakeholders such as healthcare administrators, prescribers, pharmacists, and academics is necessary. Improvement initiatives should account for the unique issues faced by the region.
Funding
The authors received no specific funding for this work
Conflicts of interest
None to disclose
Acknowledgements
Thank you to the KASIC advisory board, and antimicrobial stewardship champions everywhere, for their tireless work to improve antibiotic use. SE Moore would also like to thank Brandon J Hebert, MD for sharing his experiences in medical education; they have enriched the author’s holistic understanding of antimicrobial stewardship issues.