Introduction
The COVID-19 pandemic, caused by the novel coronavirus SARS-CoV-2, has generated a global health crisis. A substantial proportion of individuals experience ongoing symptoms and clinical sequelae, even after the infection’s acute phase resolution or after testing negative for SARS-CoV-2. This condition, known as “Long COVID”, is a debilitating, multisystem disorder, with the potential to cause a variety of symptoms, which can impair daily activities for months to years. Viewing Long COVID as a chronic condition should be prioritized, as the illness has become a significant burden on public health, and society.1–4
This review article aims to provide an overview of Long COVID, its significance as a public health concern, and the burden it imposes. It will explore the epidemiology, definition, risk factors, natural history, clinical manifestations, pathophysiology, management, and prevention strategies associated with Long COVID, focusing on the latest evidence from published literature. By synthesizing existing knowledge and identifying research gaps, this review aims to contribute to the growing body of evidence on Long COVID, guiding future research and clinical practice in addressing this emerging public health challenge.
Epidemiology
It has been three years since the World Health Organization declared COVID-19 a pandemic. Since March 2019, at least 65 million people are projected to suffer Long COVID symptoms, which is an estimated 10 to 20% of the individuals who recovered from the acute phase of COVID-19.3
In the United States, more than 40% of adults report prior acute COVID-19 symptoms, with nearly 1 in 5 (19%) of whom still experience Long COVID clinical sequelae.5 Long COVID is not limited to vulnerable populations, as even adults aged ≤50 and those without pre-existing conditions have an increased risk.2 This condition can affect the biopsychosocial aspects of individuals and communities. It was estimated that 1 out of 10 individuals who suffer Long COVID symptoms will stop working, resulting in economic losses and socioeconomic issues. Moreover, due to the lack of diagnostic tests and definition agreement, Long COVID is underdiagnosed and frequently disregarded as a psychosomatic disorder.3
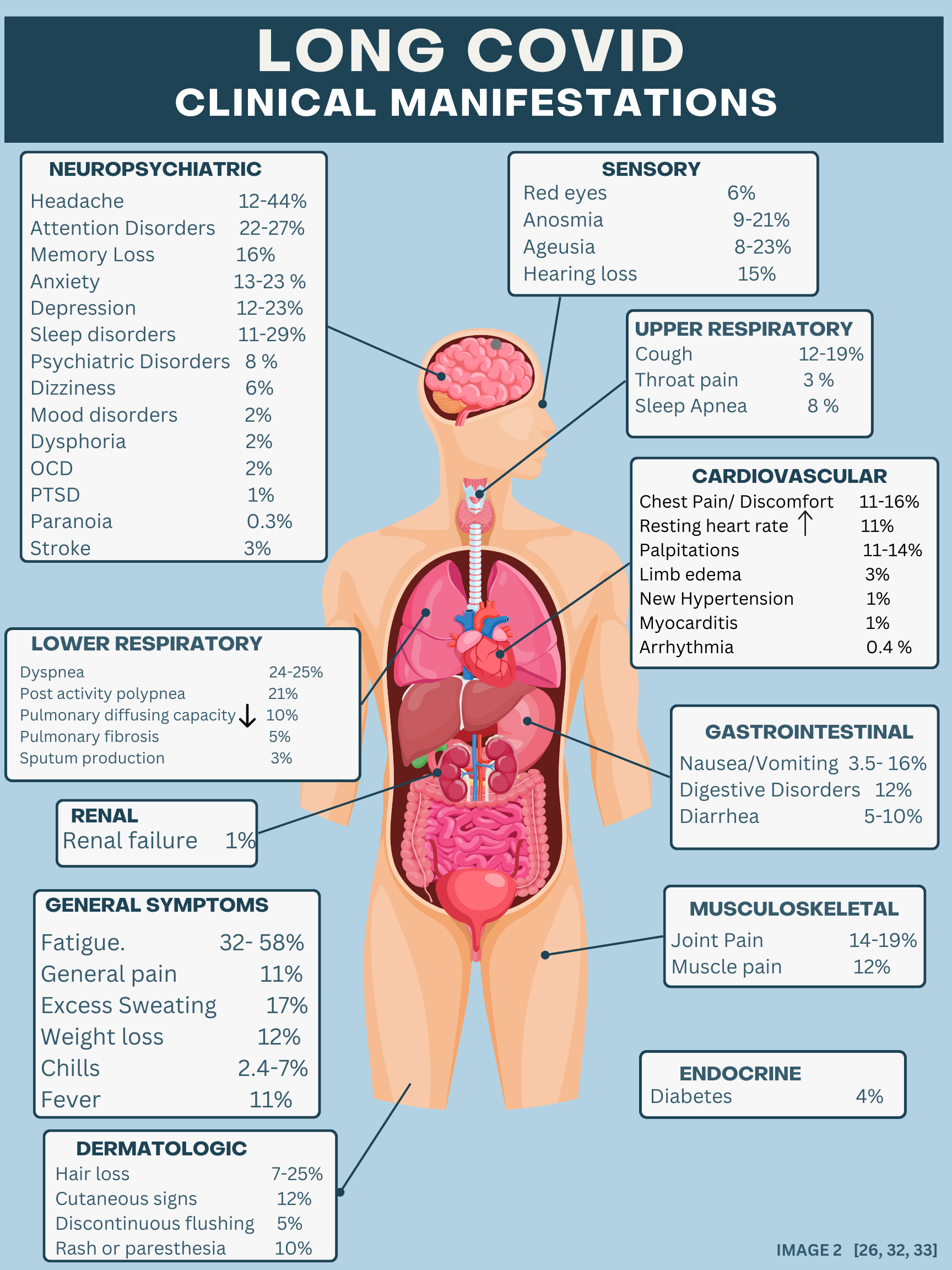
An analysis of 54 studies spanning 22 countries with 1.2 million COVID-positive individuals concluded that approximately 6.2% of individuals with symptomatic SARS-CoV-2 infection experienced at least 1 of 3 Long COVID symptom clusters three months after initial infection.1 These symptom clusters are ongoing respiratory problems, persistent fatigue with bodily pain or mood swings, and cognitive problems – all of which can significantly impact the affected individuals’ quality of life.1
Another study compared previously confirmed COVID-19-positive patients against two control groups: COVID-19-negative patients and individuals diagnosed with other respiratory viruses. They found that 14% of adults, aged 18 – 65, developed at least one Long COVID symptom that required medical attention. This is 4.95% higher compared to COVID-19-negative patients, and 1.65% higher compared to individuals diagnosed with other viral lower respiratory tract illnesses.2
Methods
A literature search was conducted through PubMed, and the Norton Healthcare library database with the following key phrases: “Long-term COVID symptoms,” “Post COVID syndrome,” “Long COVID pathophysiology,” “SARS-CoV-2 natural history,” “Long COVID definition,” “Long COVID clinical manifestations,” “Long COVID viral persistence,” “Long COVID immune system abnormalities,” “Long COVID dysregulated inflammatory response,” “Long COVID dysbiosis,” “Long COVID and viral reactivation,” “Long COVID microthrombi,” “Long COVID management.” The listed authors screened relevant abstracts to identify reviewable papers. Studies on Long COVID that included symptomatic prevalence are summarized in Table 1 and Figure 2.


SARS-CoV-2 Infection: Natural History and Definitions
Long COVID Definitions
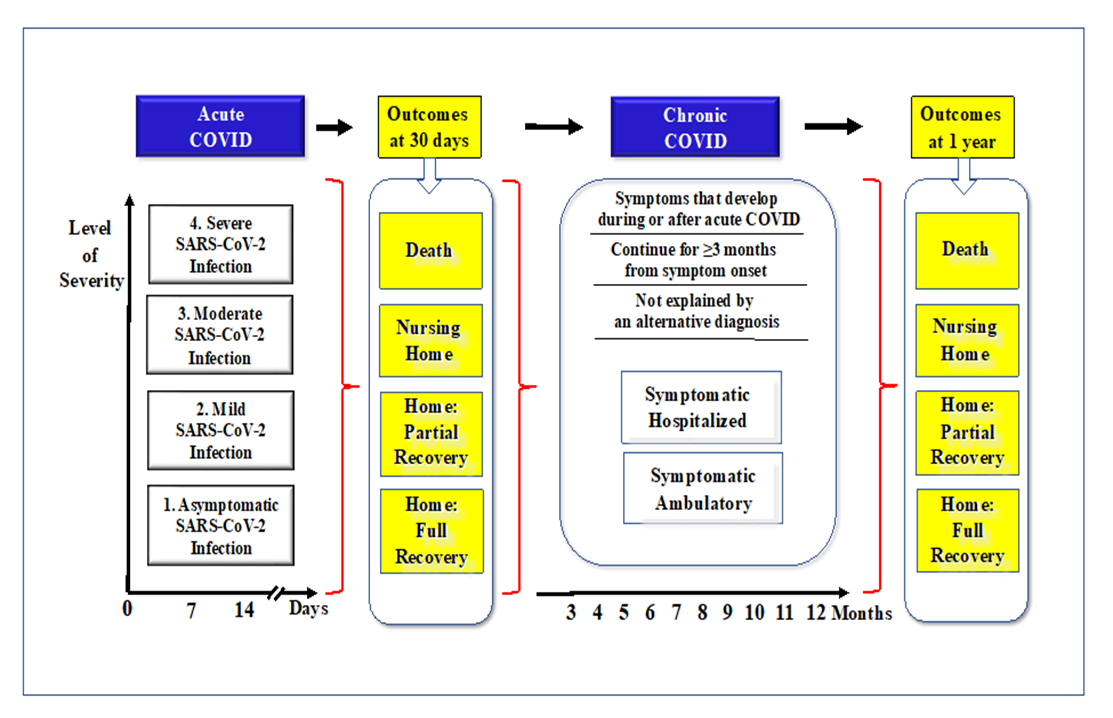
The definition of Long COVID has been evolving as more evidence becomes available. In an international panel of 265 individuals (patients, clinicians, researchers, and WHO staff), 14 domains and 45 items were evaluated in two separate rounds in order to determine an agreed-upon definition for Long COVID.8 The final consensus states that post-COVID-19 condition occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually three months from viral onset, with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis.8
Natural History of Long COVID
Acute COVID-19 infection can be categorized by level of severity and site of care. For example, mild COVID-19 cases account for ambulatory patients, moderate cases for patients admitted to hospital wards, and severe cases for those admitted to the ICU. The proportion of patients who developed Long COVID is higher among patients admitted to the ICU (43.1%) and general wards (27.5%) compared to patients with only an ambulatory status (5.7%).1
As a risk factor, Long COVID appears to be more prevalent among females compared to males. In one study 10.6% of women and 5.4% of men aged 20 years or older developed Long COVID three months after symptomatic SARS-CoV-2 infection.1 The duration of Long COVID symptoms varied, though, depending on hospitalization status. Among individuals who were hospitalized (ICU and general ward), the estimated mean duration of Long COVID symptoms was 9.0 months, while the length among those who were not hospitalized was 4.0 months.1
Of the patients who developed Long COVID symptoms that persisted for three months after initial infection, 15.1% continued to have persistent symptoms after one year; however, the long-term outcomes of post-COVID beyond twelve months are not yet well understood.1 Further research is needed to understand the natural history and prognosis of Long COVID taking into consideration long-term outcomes.
Long COVID Pathophysiology
Viral Persistence
One of the leading hypotheses for the pathophysiology of Long COVID is viral persistence in the body. This hypothesis stems from observing lingering inflammation in individuals months after symptom onset that has resulted from virally infected cells.9 A recent study published in Frontiers in Immunology studied occurrences of the SARS-CoV-2 S1 protein by analyzing monocytes, T-cells, and B-cells in patients with post-acute sequelae of COVID-19 (Long COVID). They discovered that the levels of intermediate and non-classical monocytes were elevated in Long COVID patients for up to 15 months.10 In addition to immune system viral persistence, SARS-CoV-2 has also been found in other systems such as fecal samples of the gastrointestinal tract,11 pulmonary tissue,12 and cerebrospinal fluid,13 to name a few.
Immune System Abnormalities
Another hypothesis for the pathogenesis of Long COVID involves autoimmune processes. One explanation is that SARS-CoV-2 can provoke the development of autoantibodies. A study published in the Journal of Translational Autoimmunity looked at functional autoantibodies against G-protein coupled receptors in patients with Long COVID. All 29 of their patients developed autoantibodies that disturbed vascular and neuronal processes with G-protein coupled receptors.14 Another study analyzed the impact of autoantibodies on COVID-19 progression. Results found that COVID-19 patients increased autoantibody reactivity compared to controls. Many of these antibodies were against immunomodulatory proteins such as complement components, chemokines, cytokines, and cell surface proteins.15 Autoantibodies against tissue-associated antigens also revealed a potential connection to Long COVID, as many of the specific autoantibodies discovered were also present in Long COVID patients.
Dysregulated Inflammatory Response
Another theory for the pathogenesis of Long COVID is a dysregulated inflammatory response. Both the innate and adaptive immune system responses to SARS-CoV-2 include clearing viral load, inhibiting viral replication, and promoting tissue repair.16 It has been proposed that after invading the host, SARS-CoV-2 can promote continued stimulation of the innate immune responses, resulting in chronic inflammation in affected areas.17 Many Long COVID patients present with increased interferon-y, interleukin-2, B-cell, CD4+, and CD8+ T-cells, and also can have effector T-cell activation. This systemic inflammatory response can eventually cause chronic inflammation, in which long-term system and organ damage may occur. The pathogenesis of dysregulated inflammatory responses relating to Long COVID should be explored further in order to determine probable correlation with other theories such as viral persistence.
Dysbiosis
Dysbiosis is considered to be a disruption to the gut microbiome. Gastrointestinal problems, such as bloating, vomiting, diarrhea, and stomach pain have become common symptoms reported by COVID-19 patients. A large study using the US Department of Veterans Affairs national health care databases discovered that after the first 30 days of infection, individuals with COVID-19 are at an increased risk for developing gastrointestinal disorders a year later.18 Some of the main microbiota alterations seen in COVID-19 patients were beta-diversity changes, alpha-diversity reductions, and/or a connection with cytokine inflammation markers.19 Additionally, many patients present with COVID-19 biomarkers in the RNA of their feces months after infection. More research involving the pathogenesis of Long COVID should be conducted in order to determine if changes to the gut microbiome not only involve gastrointestinal symptoms but also respiratory and neurological problems.
Reactivation of other viruses (Herpes)
Many symptoms associated with Long COVID, such as fatigue, chronic stress, and anxiety are similar to Epstein Barr Virus (EBV) and other herpesviruses. A leading hypothesis to the pathophysiology of Long COVID is the reactivation of viruses, specifically EBV that have been dormant in the body.20 Decreased immune function in COVID patients allows for virus reactivation, and this co-infection could ultimately instigate Long COVID symptoms. Evidence suggests that EBV triggers SARS-CoV-2 to enter epithelial cells by inducing the expression of angiotensin-converting enzyme 2.21 Additionally, there has been an indication that T-lymphocytes infected with EBV reduce antiviral cytotoxic mitochondria function. This has been shown to cause apoptosis in the mitochondria, leading to increased myeloid suppressor cells and lymphopenia.22 One study with 185 COVID-19 patients found that 66.7% of Long COVID patients had EBV reactivation at disease onset. 18 additional patients had EBV reactivation 21-90 days after disease onset.23 More research should be conducted; however, for patients presenting with COVID-19, a previous EBV history could be predictive for long-term COVID outcomes.
Microthrombi
Several studies have proposed that the endothelium is a critical part of Long COVID’s pathophysiology.24–26 Microthrombosis, capillary integrity deterioration, reduced oxygen extraction, and capillary flow disturbance have all been shown to persist in COVID-19 patients, even when the disease is no longer detectable.27 Oftentimes, COVID-19 involves systemic hypoxia, which results in the release of cytokines. Specific cytokine inflammatory factors, like TNF-alpha, damage epithelial functions and topical oxygen levels in many different organ systems.27 As a result, hypoxia-inducible transcription factors are activated to help the body adapt to new oxygen levels. A state of hypoxia also instigates an inflammatory response, as it stimulates the production of the nuclear factor kappa beta.27 COVID inflammation combined with prior and/or stimulated capillary damage can thus interfere with the oxygenation of blood tissue. This interference is ultimately the hypothesis behind microthrombi Long COVID complications.
Long COVID Management
General Recommendations
Clinical practice has currently embraced a symptom-based approach to Long COVID management. A complete assessment including full blood count, renal function, C-reactive protein, liver function test, thyroid function, hemoglobin A1c, vitamin D, magnesium, B12, folate, ferritin, and bone studies should be conducted. Additionally, a thorough medical history and examination should take place in order to ensure symptoms are not being caused by a non-COVID-related diagnosis.28 Medical professionals are giving their best efforts to implement and promote guidelines on Long COVID management, yet there are gaps in diagnosis and treatment.
General Long COVID recommendations are entirely dependent upon laboratory results and clinical symptoms. For example, patients presenting with cardiopulmonary symptoms are recommended to receive chest imaging and electrocardiography, and pulmonary function tests.28 For those presenting with dyspnea and or pulmonary rehabilitation, oxygen supplementation is recommended. Patients with Long COVID can present with a wide range of symptoms that can last for weeks, months, and/or years. Due to the individualized nature of this chronic condition, it is important that healthcare providers properly diagnose patients in order to give them appropriate care and treatment.
Research Considerations
More research is needed to properly understand Long COVID management. Data on the management of Long COVID symptoms remains limited, and a standard of care has yet to be established. No one test can diagnose Long COVID, and current management processes are solely research considerations.
Some of the recommendations for the management of immune system abnormalities in Long COVID include immunomodulatory therapies.29 As symptoms progress to a chronic state, research suggests that immunosuppressive treatments could be beneficial.29 For more severe cases, clinical trial therapies such as rituximab, extracorporeal apheresis, plasmapheresis, and intravenous immunoglobulin could be considered.29 Dexamethasone has frequently been utilized to treat inflammation in acute COVID, but may also be beneficial in preventing long COVID symptoms according to an eight month follow-up observational study.30
For patients with underlying cardiac or pulmonary disease, pharmacological therapy can be utilized. In an observational study published in the Annals of the American Thoracic Society, nearly 5% of 837 patients with post-acute COVID infection were found to have interstitial lung disease, such as organized pneumonia, which resulted in symptomatic and radiological improvements after treatment with oral corticosteroids.31
Probiotics are live microorganisms that can help diversify gut microbiota in order to help the body potentiate immune responses, bind to pathogens, and maintain epithelial barriers.32 One clinical study found that consuming probiotics after contracting COVID-19 could reduce the possibility of secondary infection, relieve COVID-19 symptoms, as well as boost the immune system.33 Another randomized clinical trial looked at the efficacy of probiotics on COVID-19 outpatients. A negative RT-qPCR test as well as symptom clearance was assessed. The probiotic group achieved these results 53.1% higher than the control group.34 While current data is limited to acute COVID-19 infection, the authors suggest that emerging research topics should focus on the use of probiotics in managing long-term COVID dysbiosis.
Less is known in regards to the treatment of Long COVID symptoms as a result of viral reactivation; however, many antiviral treatment therapies utilized for acute COVID may prove beneficial. Ganciclovir, an anti-herpes drug and nucleoside analog, inhibits EBV viral replication by DNA polymerase and has been shown to reduce mortality in severe COVID patients. The inhibition of viral replication and an overall decrease in viral load may result in improved outcomes for patients with acute and long COVID.35
It is unknown how long a hypercoagulability state may persist in long COVID patients, and the majority of post-acute COVID patients who received anticoagulation therapy in the hospital prophylactically, with no evidence of thromboses, are discontinued from their therapy upon discharge. There is currently a multitude of randomized drug studies being completed globally, according to ClinicalTrials.gov, that are researching the indications, risks, and benefits of post-discharge thromboprophylaxis therapy.
Exercise has also been proposed as a management method for post-COVID immune system abnormalities. Strength and aerobic training in particular have been found to improve pain, increase quality of life, and boost physical function. More research in cardiovascular health-related immune abnormalities should be conducted to further understand the clinical manifestations of post-COVID syndrome.
Long COVID Prevention
Clearly, the most effective manner in which to prevent Long COVID is to control SARS-CoV-2 infection by means of vaccination, social distancing, masking, and frequent hand hygiene.34 By collectively implementing these infection prevention strategies, the incidence of long COVID may be reduced. Certain pharmacotherapy treatments used in acute COVID may also be beneficial in the prevention of Long COVID. A preclinical study published in the Journal of the American Medical Association concluded that molnupiravir, an oral medication used under emergency use authorization for the treatment of mild to moderate COVID, was effective in attenuating Long COVID symptoms. Immunomodulating drugs, specifically monoclonal antibodies such as infliximab and leronlimab, are also being analyzed. Studies have also shown antihistamines may prove effective in relieving persistent symptoms. Other preventative measures include prebiotics and probiotics, increased physical activity, and diet modification.35
Conclusions
Long COVID is a complex condition that can significantly impair daily activities and quality of life. This illness presents with a wide array of clinical manifestations involving multiple organ systems. Management of Long COVID is currently based on a symptom-based approach in which providers must collaborate with other healthcare professionals to rule out competing diagnoses. Thus, recognizing and understanding Long COVID’s symptoms and clinical manifestations is crucial for accurate diagnosis and appropriate management of the condition.
The pathophysiology of Long COVID is complex and not yet fully understood. It most likely involves a combination of hypotheses relating to viral persistence, immune system abnormalities, dysregulated inflammatory response, dysbiosis, reactivation of other viruses, and microthrombi formation. These mechanisms contribute to the complex nature of Long COVID and its diverse range of symptoms. Understanding these mechanisms and their correlations are crucial for developing effective management strategies.
In conclusion, Long COVID is a significant challenge to global public health. The wide range of symptoms and potential long-term implications it imposes on individuals, healthcare, and society has created a silent pandemic. Raising awareness of Long COVID by understanding its natural history, prognosis, and pathogenesis is imperative towards developing effective treatment guidelines for this emerging healthcare burden.