





Introduction
Mycoplasma pneumoniae has been identified as a cause of respiratory infections in children, adolescents and adults. Infections of M. pneumoniae can lead to severe disease with pneumonia requiring hospitalization.1–6 M. pnuemoniae has a slow incubation period of 1-4 weeks, with cyclic epidemics every 3-5 years,7,8 followed by periods of decreased transmission due to development of transient population immunity.
A decrease in M. pnuemoniae infections was noted during the COVID-19 pandemic, likely due to heightened use of non-pharmacologic interventions such as social distancing, masking, and decreased exposure to large groups3,9–14 Following the COVID-19 pandemic, a re-emerging of M. pnuemoniae infections was noted globally since the end of 202310,15–21
Outbreaks of M. pneumoniae can be prolonged due to the slow incubation period. The potential for prolonged M. pnuemoniae outbreaks has important implications for infection prevention practices in healthcare, long term residential facilities, and community settings. Rapid recognition and characterization of M. pneumoniae outbreaks is important for the development of infection prevention strategies in these settings.
We recently published a manuscript describing an outbreak of M. pnuemoniae infections in the United States.22 This manuscript reviewed electronic medical records from over 280 million patients across the US. To further assess the outbreak at a local level, we analyzed data from the Norton Healthcare system in Louisville, Kentucky. The purpose of this study is to describe the epidemiology and characteristics of patients with M. pneumoniae infection in Louisville, and to review the clinical practice and public health implications of this outbreak.
Methods
Study design and patient population
This was a retrospective study of patients in Louisville, Kentucky seeking care at a Norton Healthcare. Norton Healthcare includes five hospitals and over forty primary care facilities, immediate care centers, and prompt care clinics.
Inclusion criteria
Patients were included in this study if they had a positive nucleic acid amplification test (NAAT) for M. pneumoniae at a Norton Healthcare hospital or clinic between January 1, 2017 to December 31, 2024.
Patient characteristics
Patient demographics, past medical history, need for hospitalization, and need for ICU stay were abstracted from electronic medical records.23 Past medical history was defined by ICD-10 codes (see supplemental materials).
Baseline data
To assess the current outbreak, patients with M. pneumoniae infection from January 1, 2017 to March, 31 2020 were grouped into a baseline study cohort. Electronic medical records to review patient demographics and past medical history were available for patients beginning in January 1, 2018.
Current outbreak
The current infection period was defined as October 1, 2023 to December 31, 2024. To identify the presence of an outbreak, patients were aggregated in annual quarters and depicted in count charts (c-charts). Expected control limits were derived from the baseline cohort using the baseline mean and standard error, with the upper control limit (UCL) set at 3 SE above the mean. The presence of an outbreak was defined as any quarter above the baseline UCL. Additional c-charts were created for pediatric (age < 18) and adult (age ≥ 18) patients.
Statistical analysis
Patients’ characteristics were reported for the baseline cohort and current outbreak and depicted as frequency and percent. Chi-squared tests of independence were performed to assess differences in patient characteristics.
Results
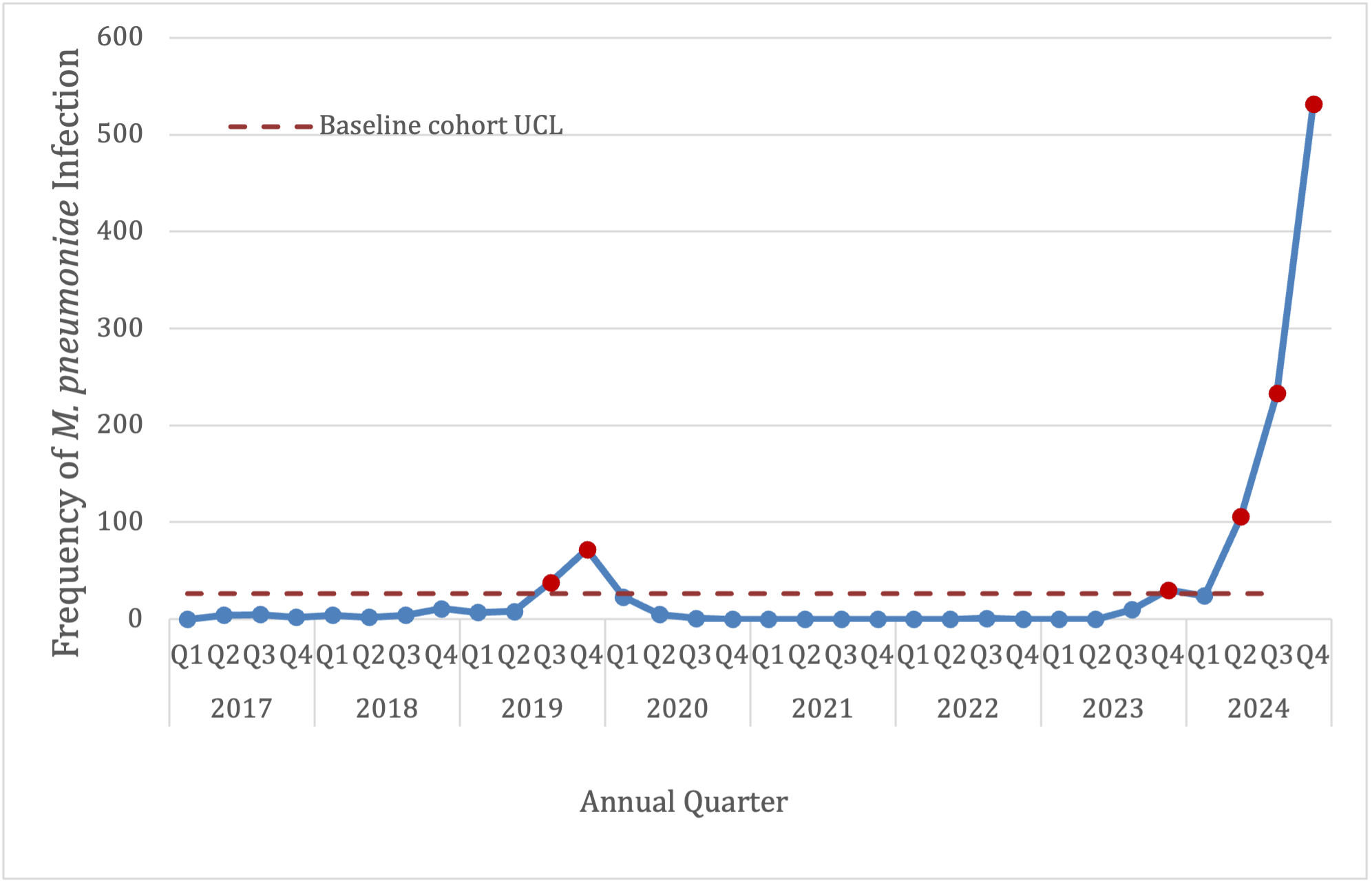
The epidemic curve for all patients with M. pnuemoniae infection is depicted in Figure 1. The current outbreak started in the fourth quarter of 2023, with cases in excess of the upper control limit climbing through the end of 2024. The current outbreak included a total of 925 patients.

During the current outbreak, testing for M. pneumoniae and percent positivity increased. Percent positivity peaked during the current outbreak at 6%. For the baseline cohort, percent positivity peaked at 2%. The percent positivity by tests are depicted in Figure 2.

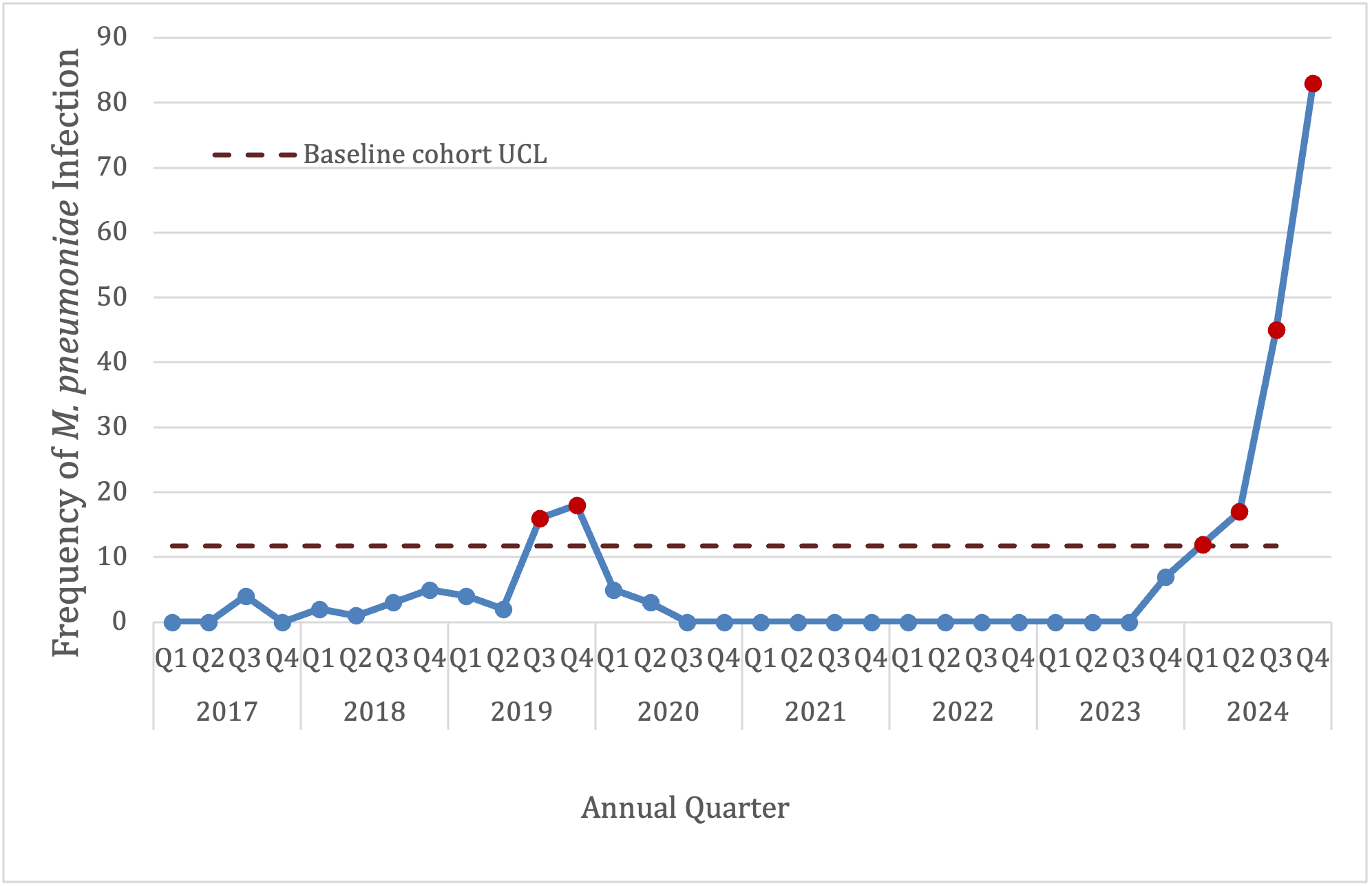
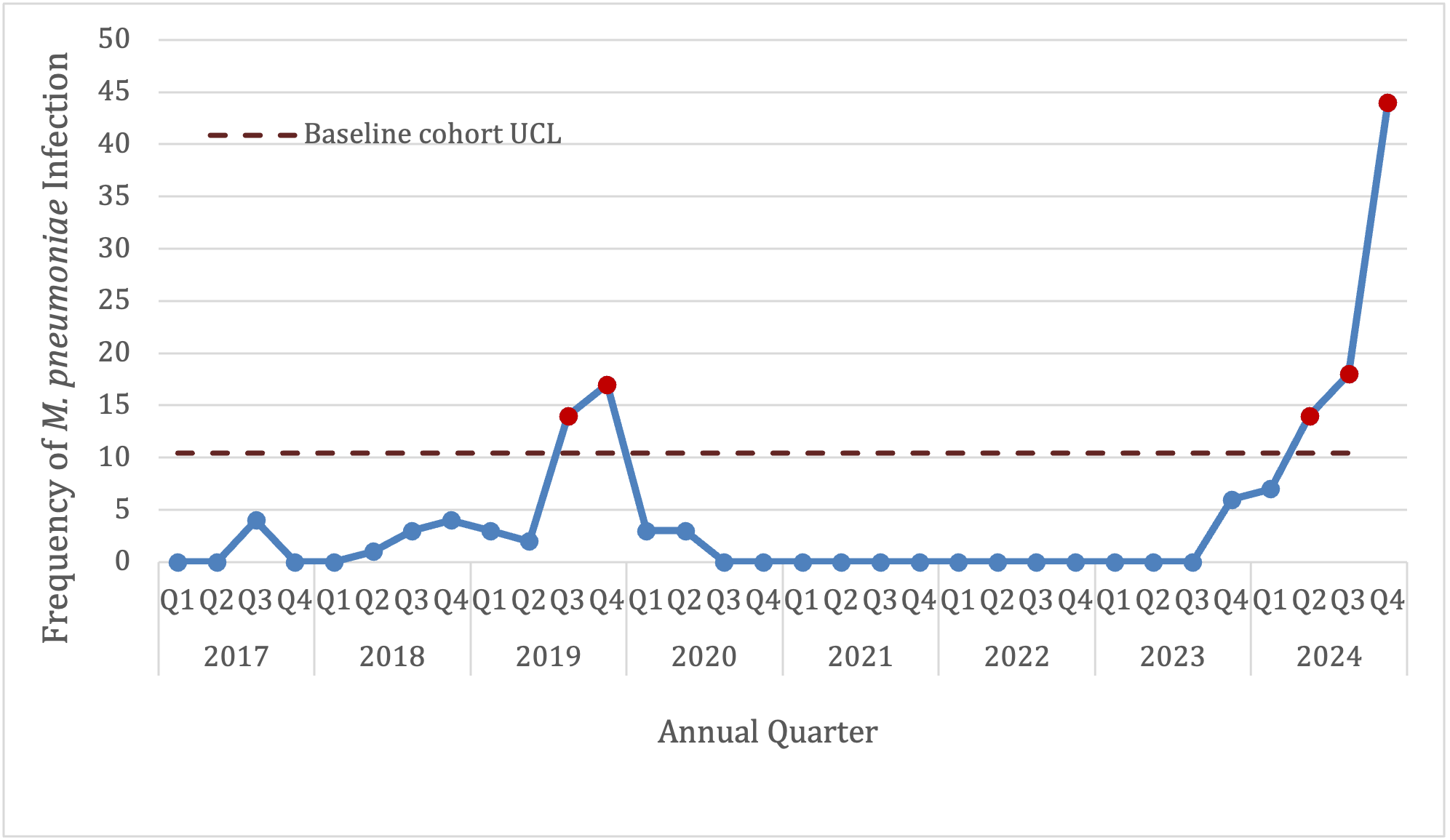
In the current outbreak, a total of 761 pediatric patients, and 164 adult patients had M. pneumoniae infection. The epidemic curves for pediatric patients and adult patients with M. pnuemoniae infection are depicted in Figures 3 and 4, respectively.


During the current outbreak, M. pneumoniae infections led to hospitalization in 243 patients. Of these, 154 pediatric patients were hospitalized and 89 adult patients were hospitalized. The epidemic curves for all patients hospitalized with M. pnuemoniae infection, pediatric patients hospitalized with M. pnuemoniae infection, and adult patients hospitalized with M. pnuemoniae infection are depicted in Figures 5, 6, and 7, respectively.



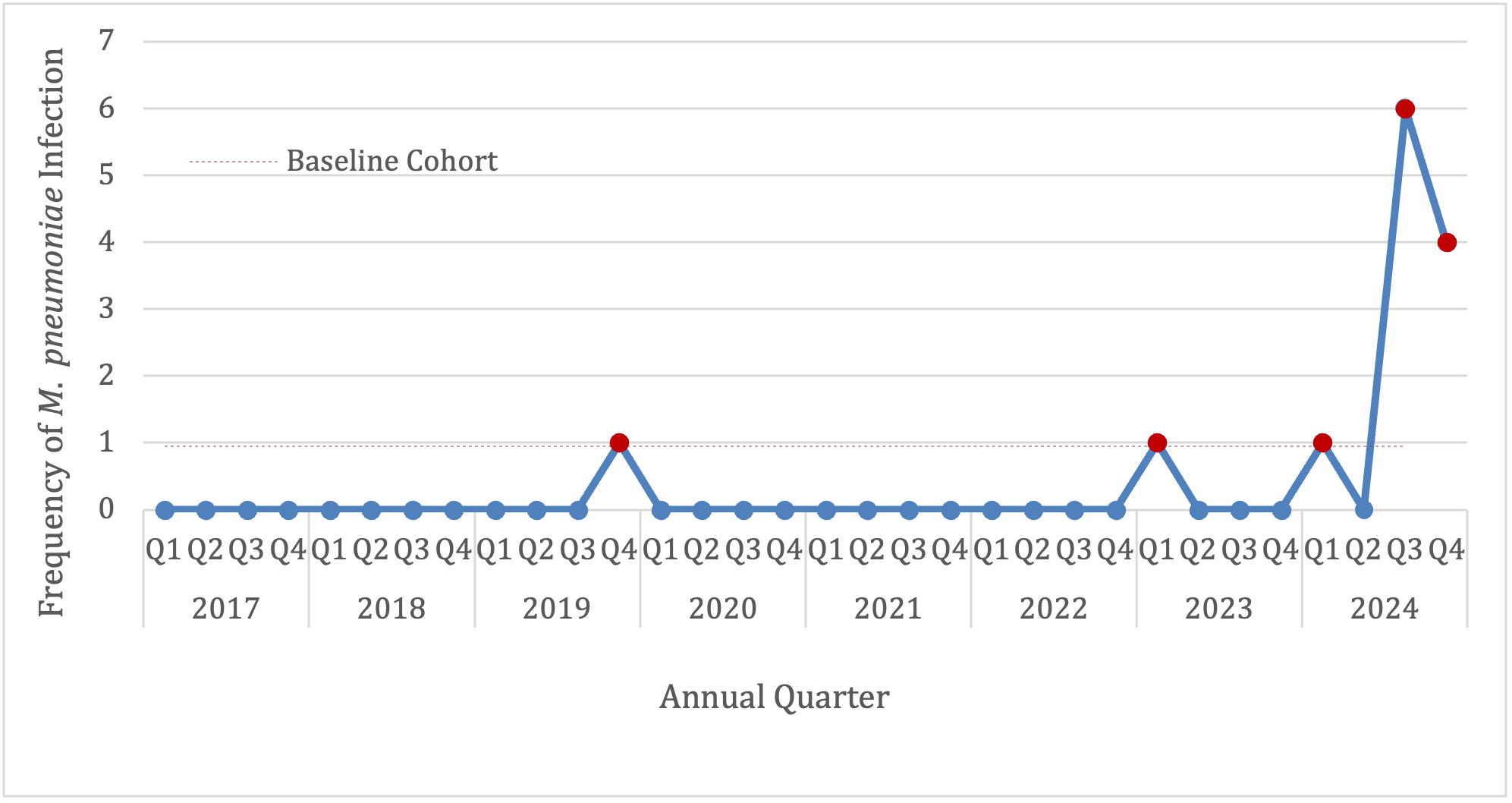
Of patients hospitalized with M. pnuemoniae infection, severe infection requiring ICU stay was observed in 60 patients during the current infection period. A total of 49 hospitalized pediatric patients and 11 hospitalized adult patients required ICU stay during the current infection period. The epidemic curves for all patients, pediatric patients, and adult patients requiring ICU stay are depicted in Figures 8, 9 and 10, respectively.



Patient characteristics for pediatric and adult patients with M. pnuemoniae infection are presented in Tables 1 and 2, respectively. Patient demographics and past medical histories were similar between the baseline and current infection periods for both pediatric and adult patients.
Discussion
This study describes an ongoing outbreak of M. pnuemoniae infection in adults and children in Louisville, KY, USA. Excess infections of M. pneumoniae have been observed starting in the third quarter of 2023 and have continued to the present. When we compare the current outbreak with the baseline M. pneumoniae infections in Louisville, we see an increase in the number of infections requiring hospitalization and also requiring need for ICU admission. This data suggests an increased severity of infections with M. pneumoniae. When we compare the population characteristics of pediatric and adult patients in the current outbreak with those in the baseline cohort, we did not observe any significant differences. The increased severity of the current outbreak cannot be explained due to a population that is more prone to poor outcomes, such as those who are immunocompromised or have multiple comorbidities. It may be speculated that the increase in severity of disease during the current outbreak is due to changes in M. pneumoniae virulence or a significant decrease in M. pneumoniae immunity due to the occurence of the COVID-19 pandemic.
During the COVID-19 pandemic, the use of polymerase chain reaction (PCR) for diagnosis of SARS-CoV-2 became standard of practice. After the pandemic, PCR detection for respiratory pathogens is more frequently used across the country. Increased detection of respiratory pathogens after the COVID-19 pandemic can be explained in part due to increased diagnostic testing. In this study, to compensate for this, we compared the number of tests to test positivity. Despite the increased number of tests, the test positivity still rose to 6%, triple the percent positivity of the baseline cohort, during peaks of the current outbreak, indicating that an increase in the number of tests was not solely responsible for the increase in observed infections.
Implications of the results
In this context, the current outbreak of M. pnuemoniae has implications for clinical practice. There is need for a low threshold for respiratory NAAT/PCR panel testing to better define the etiology of respiratory infections. Since M. pneumoniae does not respond to beta-lactam antibiotics ,24 clinicians should consider the possibility of this atypical pathogen when prescribing antibiotics to patients with respiratory illness. There are also public health implications since guidelines for infection prevention in patients hospitalized with M. pneumoniae recommend both droplet and standard precautions for the duration of illness.25 Consistent use of standard precaution measures such as frequent hand washing with soap and water, use of an alcohol-based hand sanitizer, and covering coughs or sneezes are essential to help prevent disease spread in community setting..
M. pneumoniae antimicrobial postexposure prophylaxis has been explored in close contact settings, such as hospitals, residential institutions for special needs populations, and military training facilities.26–29 A randomized, double-blinded placebo-controlled trial conducted among asymptomatic hospital employees during a M. pnuemoniae outbreak showed fewer episodes of clinically significant respiratory illness in the azithromycin group compared to placebo.27 Observational studies of M. pnuemoniae outbreaks in residential facilities for developmentally disabled adults demonstrated a significant reduction in the secondary attack rate and rapid outbreak cessation with the combined use of azithromycin prophylaxis and strict infection control measures.26,29 Weekly oral azithromycin was found to be superior in preventing respiratory infection compared with intramuscular benzathine penicillin G prophylaxis, in a double-blind placebo controlled study of Navy Special Forces trainees, where M. pnuemoniae accounted for approximately 16% of acute respiratory infections.28
Our findings align with recent literature in the area of M. pneumoniae infections. An increase in M. pnuemoniae in children and adolescents was reported in the fall of 2023.10 Subsequently, an overall increase in M. pnuemoniae test positivity observed across age groups, prompted a Centers for Disease Control and Prevention (CDC) alert in October of 2024.18
Norton Healthcare is the largest healthcare system in the city of Louisville, which represents approximately 60% of the market share for inpatient visits and clinic visits in the city of Louisville. This indicates that our study results are more likely generalizable to the full Louisville community.
Future research may look at isolation of M. pneumoniae to define any change in virulence factors as well as antimicrobial susceptibility.
In conclusion, we documented a current outbreak of M. pneumoniae infections in Louisville, starting in the fourth quarter of 2023. This outbreak of respiratory infections due to an atypical pathogen has implications for clinicians and public health professionals. This outbreak highlights the importance of active surveillance of respiratory pathogens.