Introduction
The release of environmental lead during the 20th century is one of the greatest environmental disasters in recorded history.1 Lead is a known environmental neurotoxicant and can negatively impact almost every aspect of human health.2 Early life lead exposure has been associated with hearing loss, speech problems, renal insufficiency and failure, hypertension, heart disease, problems with reproduction, and reduced adult brain volume.3 Further, it is currently believed that the most common type of lead exposure in the United States (US) is chronic low-level exposure with subclinical symptoms that may manifest later in life as learning difficulty, poor school performance,4 and/or behavioral problems.5
While lead does not serve a single biological function for the human body,6 childhood lead poisoning still affects thousands of children each year in the US.7 The most recent National Childhood Blood Lead Surveillance Data published by the Centers for Disease Control and Prevention (CDC) reported 726,850 children had confirmed blood lead levels > 5 mcg/dL between 2012 and 2018. However, this report is an under representation of the true number of children with an Elevated Blood Lead Level (EBLL), as 20 states failed to return complete surveillance data for the entire time period. Additionally, of these 20 states, 8 did not submit any blood lead surveillance data.8 While Kentucky (KY) submitted data for each year, some of the years appear to be incongruent with county level data. For example, 2016 surveillance data for Jefferson County, KY (Jefferson County) showed 0 children with a blood lead level > 5 mcg/dL.8 This appears to be inconsistent with blood lead surveillance data collected by the Louisville Metro Department of Public Health and Wellness (LMPHW). Blood lead surveillance data from the LMPHW’s most recent Health Equity Report showed 1,413 children with a reported blood lead level > 5 mcg/dL between 2011 and 2016.9
While local and state blood lead surveillance data for Jefferson County is of record, currently no report has conducted an epidemiological investigation on all known and available county-level blood lead surveillance data. Additionally, local and state reports are based upon the prior CDC Blood Lead Referent Value (BLRV) of > 5 mcg/dL, which was recently lowered to > 3.5 mcg/dL on October 28, 2021.10 To address these issues, our report put together the largest known blood lead dataset for Jefferson County with the goal of providing a more thorough county-level description of childhood lead levels. The primary purpose of our report is to provide medical and public health professionals information on the magnitude and spatiotemporal distribution of childhood lead levels within Jefferson County.
Methods
This report was created from all available pediatric blood lead data collected for Jefferson County, KY between December 21, 2005 and June 25, 2021. This data was either reported directly to the Louisville Metro Department of Public Health and Wellness (LMPHW) and/or to the Kentucky Cabinet for Health and Family Services. This research has received approval from our Institutional Review Board (IRB: 22.0509).
Statistical Analysis
The final dataset used for descriptive analysis included 111,065 rows of data with at least one unique patient identifier, as well as a blood lead level > 0 mg/dL. For some children with either an EBLL or who were considered at-risk for environmental lead exposure by their medical provider, multiple blood lead levels were obtained. The data contain at least one measurement for 74,014 unique children. For the purposes of this report, an EBLL is defined as > 3.5 mcg/dL, the current BLRV established by the CDC.10 Tables including and excluding serial tests are included in the results section of this report. The exclusion of serial tests was carried out by sub-setting the original dataset on the highest blood lead test for each child in the original dataset. Stratification by race is based upon CDC definitions and includes: White, Black, Asian, Hawaiian/Pacific Islander, and American Indian or Alaskan Native.11 Data on ethnicity was not available for review. Biological sex is defined as male or female. Gender identity was not available for review. Data on health insurance type was available for review.
Descriptive analysis included the number (percentage), mean (standard deviation), and the range of blood lead tests. Unadjusted Risk Ratios (RR) were also calculated by specific demographics. Statistical significance for these RR was evaluated by the 95% Confidence Interval (95% CI). All statistics were calculated with R version 4.1.3.
Geospatial Mapping and Cluster Risk Analysis
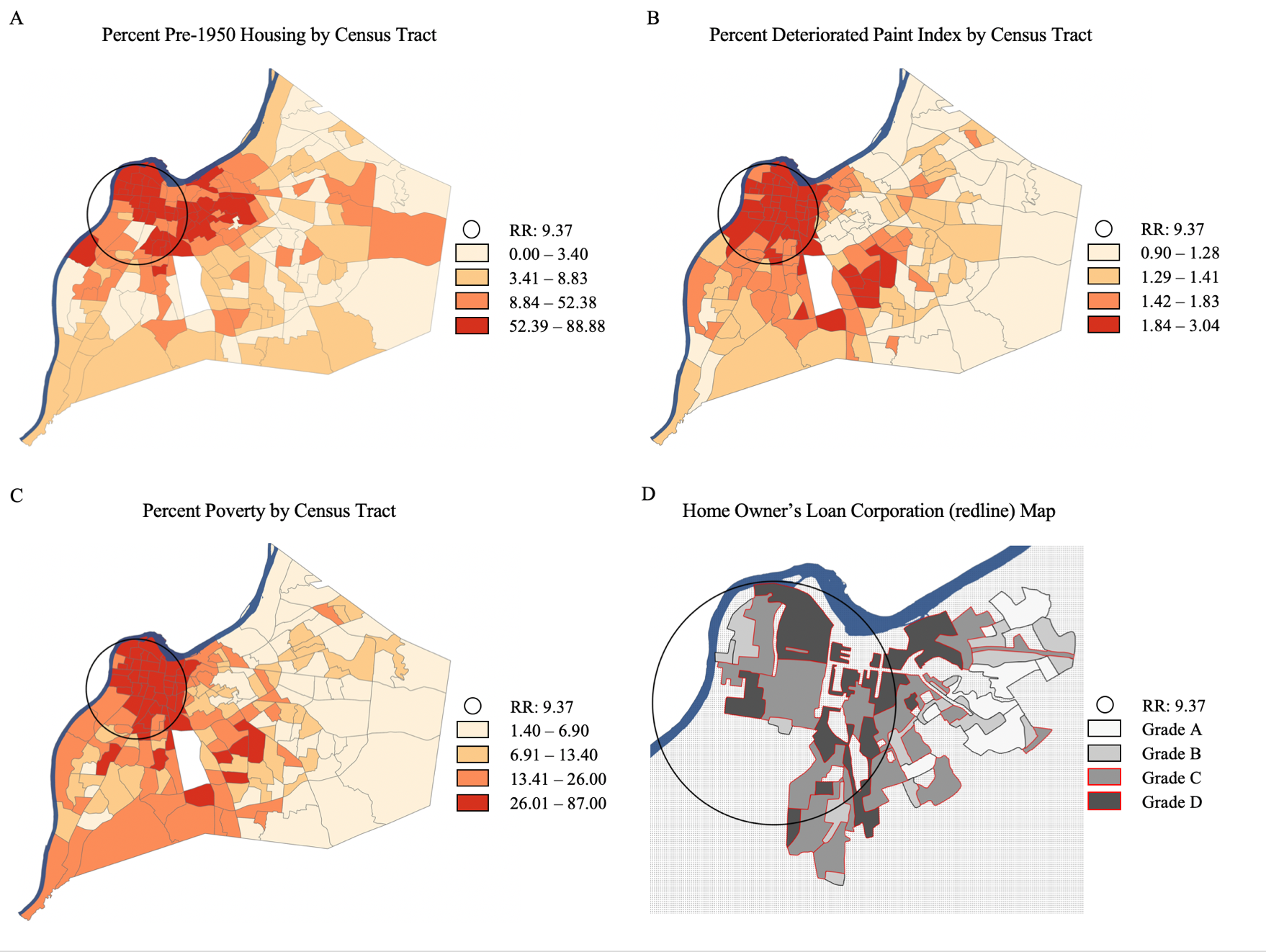
Shapefiles of Jefferson County were downloaded from the US Census Bureau’s TIGER/Line Shapefile repository. Percent poverty and percent pre-1950 housing data was downloaded from the US Census Bureau’s American Community Survey, 2016 5-year estimates. Poverty12,13 and pre-1950 housing14 are well-established risk factors for remnant environmental lead hazards. The Deteriorated Paint Index (DPI) and Home Owner’s Loan Corporation data was downloaded from the Louisville/Jefferson County Information Consortium (LOJIC). The DPI is a tool used by the US Department of Housing and Urban Development to evaluate the condition of lead-based paint in occupied homes.15 For the purposes of this report, DPI is reported as the estimated percentage of occupied homes with the potential for lead dust from deteriorating remnant lead paint. Choropleth maps were created by quantiles (Map Panels: A-C). Mapped data from the Home Owner’s Loan Corporation was produced by historical property appraisal data (Map Panel: D). All maps were produced in ESRI ArcGIS Pro version 2.8.4.

Geographic cluster analysis for Elevated Blood Lead Levels (EBLLs) was produced by the Kulldorff spatial scan statistic in SaTScan version 10.0.1. This analysis was based upon all available data with a complete and valid home address within Jefferson County. Home addresses listed as a P.O. box were excluded from this cluster analysis. All duplicate home addresses meeting the aforementioned inclusion criteria were used in this analysis. Duplicate addresses represented either a child with more than one blood lead test, siblings, or different families over time. Because home addresses were not systematically collected until 2012, the dataset for cluster analysis was reduced to 44,285 rows of data.
Results
Excluding serial tests, between 2006 and 2012, city and state blood lead surveillance systems collected an average of 7,014 blood lead tests per year. Beginning in 2013, these surveillance systems collected a reduced average of 2,972 blood lead tests per year. In fact, from 2012 to 2014, there was a 57% reduction in blood lead tests reported to the appropriate public health surveillance system. Even so, our final dataset for evaluation included 111,065 blood lead tests reported between December 21, 2005 and June 25, 2021. Of these tests, which included multiple observations for children with serial testing, 16,204 (14.5%) tests registered blood lead levels > 3.5 mcg/dL. Removing serial tests from the final dataset returned 74,014 unique children with a reported blood lead test. Of these unique children, 9,823 (13.2%) had at least one blood lead test > 3.5 mcg/dL (Table 1).
Reported blood lead levels ranged from 0-100 mcg/dL. Excluding serial tests, 9,198 children had a blood lead level between 3.5-14.9 mcg/dL, while 625 children had blood lead levels > 15 mcg/dL (Table 2). The annual EBLL prevalence rate ranged between 7.6% and 27.7% between 2005 and 2021 (Table 2). Of the 9,823 children found with an EBLL, 2,527 (25.7%) had two or more reported blood tests > 3.5 mcg/dL. Within this group, 113 children had 10 or more reported blood tests > 3.5 mcg/dL (Table 3). The most common ages for an EBLL was between 12 and 35 months (Table 4).
EBLLs impacted every racial demographic, albeit disproportionately so for some groups (Table 5). Excluding serial tests, Black children had a 77% increased risk for an EBLL compared to white children (Unadjusted Risk Ratio: 1.77; 95% CI: 1.61, 1.95). Biological males also had a 12.5% increased risk for an EBLL (Unadjusted Risk Ratio: 1.12; 95% CI: 1.08, 1.16). Additionally, children with Medicaid health insurance had more than a 3-fold increased risk for an EBLL compared to children with private insurance (Unadjusted RR: 3.73; 95% CI: 3.11, 4.47) (Table 6).
Results from the Kulldorff Spatial Scan statistic found an area of increased risk for EBLLs in the northwest corner of Jefferson County. Children within this area were more than 9-times more likely to have an EBLL compared to children who lived outside of this area (RR: 9.37; p-value: < .0001). Of the 44,285 rows of data with a valid address within Jefferson County, 7,252 (16.3%) were associated with a blood lead test > 3.5 mg/dL. Of the 7,252 mapped addresses with an associated EBLL, 4,847 (66.8%) were within the area of increased risk. The results of the Kulldorff Spatial Scan statistic appear to be spatially correlated to percent pre-1950 housing, percent DPI, percent poverty, and neighborhoods identified in 1937 as having a higher mortgage security risk per the Home Owner’s Loan Corporation (Map).
Discussion
Childhood lead poisoning remains an important public health issue in Jefferson County. From December 21, 2005 through June 25, 2021, at least 9,823 children were found to have an EBLL per the CDC’s current BLRV of > 3.5 mcg/dL. However, this number is likely an under representation of the true value, as testing and/or reporting systematically diminished after 2012. In fact, between 2012 and 2014, the number of reported blood lead tests fell by 57%. This reduction in testing and/or reporting is inconsistent with the level of risk to this pediatric population. One potential explanation for the apparent reduction in testing may be the CDC’s 2012 fiscal budget which cut funds for the Healthy Homes and Lead Poisoning Prevention Program from $29 million to $2 million. This budget cut limited, and in many cases, eliminated grants to state and local health departments for lead poisoning prevention, including testing and surveillance.16 These funds were not fully re-instated until 2018.17 The sustained reduction in testing in 2020 and 2021 was likely in part due to the COVID-19 pandemic, which saw a significant reduction in childhood lead testing nationwide in primary care settings.18 While decreased funding and the COVID-19 pandemic may have adversely impacted surveillance, the annual EBLL rate among those tested since 2007 has ranged between 7.2% and 15.8%. During the last five years of available data, the annual prevalence of EBLLs has exceeded 10% each year (Table 1). This suggests an ongoing and seemingly unabated environmental lead hazard in Jefferson County.
Of the children with an EBLL, 625 (6.3%) had blood lead levels > 15 mcg/dL. Per Kentucky Revised Statute (KRS) 211.905, any child 72 months of age or younger found with an EBLL of > 15 mcg/dL must have their primary residence investigated for potential lead-based hazards. This mandatory action extends to any structure where the child spends six or more hours per week. Homeowners must correct any identified lead hazards within 60 days of the written notification of the identified lead hazard.19,20 While KRS 211.905 addresses environmental lead hazards for some, most children with an EBLL do not exceed this threshold for mandatory action. In our dataset, of the children with an EBLL, 9,198 (93.6%) had a blood lead level between 3.5-14.9 mcg/dL. For these children with a lower level of exposure, a voluntary visual inspection for lead hazards in the primary residence can be conducted by the Childhood Lead Poisoning Prevention Program (CLPPP).21 Additionally, qualified applicants can have their primary residence evaluated by Lead-Safe Louisville for potential lead remediation or abatement services.22 While these services address environmental lead hazards in Jefferson County, they are not typically initiated until after a child has been found with an EBLL.
To prevent the deleterious effects of childhood lead exposure, primary prevention strategies are needed to remove all residential lead hazards before children can be exposed. There is a growing body of evidence that low level lead exposures, even at levels previously considered safe, can result in significant lead-associated neurological sequela.23–25 In fact, the National Institutes of Health – National Toxicology Program’s Health Effects of Low-level Lead monograph found sufficient evidence that blood lead levels < 5 mcg/dL result in adverse effects on cognitive function and academic achievement outcomes in the pediatric population.26 For example, among children with BLL < 5mcg/dL, every 1-unit increase in blood lead lowered math and reading scores.27 Another study found a significant association between attention deficit hyperactivity disorder and blood lead levels > 2 mcg/dL when compared to children with blood lead levels < 0.8 mcg/dL.28 While the current BLRV is > 3.5 mcg/dL and the threshold for mandatory lead hazard inspection is 15 mcg/dL, the CDC still contends that “no safe blood lead level in children has been identified.”29 Given this, it is possible that many children in Jefferson County, especially children with blood lead levels in the range of 2 to 3.5 mcg/dL, are being exposed to hazardous levels of environmental lead without regulatory guidelines for required remediation.
Results from the Kulldorff Spatial Scan statistic found an area of increased risk for EBLLs in Jefferson County. Of the 44,285 rows of data included in the cluster analysis, 7,252 (16.3%) were associated with an EBLL. Of these 7,252 addresses, 4,847 (66.8%) were within the area of increased risk (Map). This non-random distribution is likely related to the distribution of pre-1950 housing, a known risk factor for remnant environmental lead, especially lead paint (Map: Panel A).14 This point is further illustrated by the estimated percent of occupied housing with deteriorating lead paint (Map: Panel B).
Additionally, the area of increased risk appears to be spatially correlated to poverty, another known risk factor for childhood lead exposure.12,13 While there are neighborhoods in Jefferson County outside of our identified lead risk area with a high proportion of pre-1950 housing, these areas have less poverty (Map: Panel C). This suggests that financial resources allow for property owners to pay for any needed lead abatement or remediation. This also suggests that primary prevention strategies work, and that local, state, and federal agencies that subsidize lead abatement and/or remediation should evaluate plausible solutions for primary prevention.
The area of increased risk for an EBLL also likely provides insight into why Black children in Jefferson County are disproportionately impacted by remnant environmental lead. Jefferson County remains one of the most racially segregated counties in the United States, with a high proportion of Black residents living in the northwest corner of the county, an area with a high proportion of pre-1950 housing.30–32 These phenomena are likely the continued effects of the U.S. government’s Home Owner’s Loan Corporation, which systematically divested from Black families and low-income neighborhoods between 1933-1951.33 While this practice, more commonly known as “redlining”, was discontinued in 1951, its redlined districts appear to be spatially correlated to our area of increased risk for EBLLs (Map: Panel D).
Our study has several strengths worth mentioning. First, this is a descriptive review of the largest known blood lead dataset for Jefferson County. It is also the first descriptive review of Jefferson County’s blood lead surveillance data using the current BLRV of > 3.5 mcg/dL. Additionally, our findings suggest that decreased federal funding and the COVID-19 pandemic negatively impacted childhood lead surveillance following 2012. Even so, our dataset found 9,823 children with an EBLL > 3.5 mcg/dL. Finally, our study showed that children who live in the northwest corner of Jefferson County may have a 9-fold increased risk for an EBLL compared to children who live outside of this area.
There are also several limitations worth mentioning. Prior to 2012, the vast majority of blood lead tests collected on children did not include a home address. Therefore, the spatial statistics reported herein are only an estimate of the true burden of childhood lead poisoning in Jefferson County. For example, out of the 111,065 reported blood lead tests, only 44,285 included a home address. It is possible that the missing home addresses could change the results of our cluster analysis via the Kulldorff Spatial Scan statistic. Additionally, given the reduction in reported blood lead tests following 2012, our study results likely underrepresent the true magnitude of childhood lead poisoning in Jefferson County.
Additional caution should be used when evaluating our cluster analysis, as our results may lack geographic precision due to how pediatric blood lead surveillance has been performed. Current CDC - CLPPP guidelines do not recommend universal pediatric blood lead testing. While children are supposed to be screened for their risk to environmental lead exposure, CLPPP contends that only children found “at-risk” for lead exposure should undergo blood lead testing.34 Given this, it is likely that our blood lead dataset is missing data from children whose medical providers deemed “no risk” for environmental lead exposure. Finally, caution should also be used when evaluating our unadjusted risk ratios. Given the nature of the available surveillance data, we could not control for pertinent confounding variables that could attenuate the magnitude of the unadjusted risk ratios. Which is more, a significant majority of the race and insurance data was not available for review (Table 5). Because of this, the associated risk ratios should be interpreted with caution.
Childhood lead poisoning is often compounded by the fact that exposure occurs in disadvantaged neighborhoods, which can exacerbate existing inequalities.35,36 This environmental injustice can perpetuate cycles of poverty and limit opportunities for impacted individuals and communities. Every year in Jefferson County, hundreds of children are found with an EBLL. Addressing this issue will require a multi-faceted approach hinged on primary prevention strategies, as well as universal screening for all children in at-risk communities. Primary care medical professionals and health educators in Jefferson County should also utilize information found in LMPHW’s – online CLPPP Provider Tool Kit and Guide, which provides up-to-date information and resources concerning childhood lead poisoning.21 To alleviate the ill effects of lead exposure, we must prioritize prevention to create environments where all children can prosper free from the harms of remnant environmental lead.