



Introduction
Due to the introduction of antiretroviral therapy (ART) HIV became a chronic illness with life expectancy similar to HIV (-) controls. In spite of this PLWH still suffer from a high frequency of non-AIDS defining illnesses with high frequency of metabolic diseases.1–12 Recently it has been increasingly reported that PLWH on ART have increased metabolic complications like weight gain, insulin resistance, fatty liver, and metabolic syndrome.13–16 Since most of the above mentioned chronic diseases are also seen during normal aging and are highly related to chronic inflammation the name “Inflammaging” was adopted in the literature.2,4,5,9 One of the main reasons of accelerated aging on PLWH seems to be related to chronic inflammation and persistent immune activation but the ultimate culprit remains largely unknown and has been debated extensively in academic environments.
From all the metabolic complications weight gain has become a significant concern in the use of antiretroviral therapy (ART), both for patients and healthcare providers. It has garnered considerable attention in medical discussions, stirring debate over its underlying causes. Although some attribute weight gain and related metabolic issues in people living with HIV (PLWH) to a “return to health” following the initiation of ART, this explanation is not entirely satisfactory. ART has been independently associated with the emergence of diabetes in certain cases, which complicates the narrative.17 In examining the structural changes in fat tissue, known as lipodystrophy, it’s important to differentiate between lipoatrophy, typically linked to older NRTIs like Stavudine, Zidovudine, and Didanosine, and lipohypertrophy, often seen with some newer antiretrovirals like integrase inhibitors.18 Occasionally, patients may exhibit both conditions depending on previous exposures. For the purposes of this review, ‘weight gain’ refers to overall increases in the body fat mass without distinguishing between lipohypertrophy and obesity both of which are sometimes difficult to differentiate. It’s worth noting that fat hypertrophy doesn’t always mean obesity; it can manifest as an increase in visceral adipose tissue (VAT) or abdominal fat, even if the body mass index (BMI) doesn’t exceed 30. It’s important to recognize that BMI can underestimate adiposity in PLWH since there may be considerable muscle mass loss.
Data about the exact pathophysiology of weight gain and other metabolic complications on PLWH on the new antiretroviral drugs are lacking. Some of the proposed theories to explain those findings are:
-
Some Integrase strand transfer inhibitors (INSTI) may interfere with appetite regulation (https://www.natap.org/2019/CROI/croi_64.htm)
-
ART or the HIV itself through chronic inflammation may interfere with insulin signaling (see below section).
-
Since new antiretrovirals are much more effective in lowering the viral load it was proposed that new antiretrovirals will decrease the energy expenditure of patients, hence, increasing weight. (https://www.natap.org/2019/CROI/croi_64.htm).
-
Weight gain may reflect “Return to health”
-
Overlapping epidemics: HIV, obesity, and poverty in the US with more easy access to ultra-processed food since it affects more certain minorities (https://www.natap.org/2019/CROI/croi_64.htm)
-
Baseline obesity prior to ART may predispose to chronic inflammation (increase IL-6, sTNF-alpha32, and sCD163) and more weight gain once ART are started (https://www.natap.org/2019/CROI/croi_64.htm).
-
Immune activation at the adipose tissue level can lead to mitochondrial dysfunction, fibrosis, reduced adipogenesis, decreased production of adiponectin and leptin, and increased production of proinflammatory cytokines17 all related to the genesis of obesity.
-
HIV proteins Vpr, Nef, and Tat can affect fat metabolism once released from locally adipose tissue infected cells.17 Of note, those proteins also are capable of producing HIV-associated mitochondrial dysfunction (HIVAMD) of fat tissue.
-
There is an increase of ectopic fat distribution (more hepatic, visceral, epicardial, and muscular fat)(https://www.natap.org/2019/CROI/croi_64.htm)
-
Immune-senescence within the adipocyte local environment with lack of apoptosis and continuous growth.
-
Virological, immunological, demographic, and social factors (female sex, black race, older age, lower naïve CD4, and higher viral load all were associated to weight gain) (https://www.natap.org/2019/CROI/croi_64.htm).
-
Changes in lipid trafficking and storage.17
Is Insulin Resistance and Hyperinsulinemia Always Necessary for Weight Gain on PLWH?
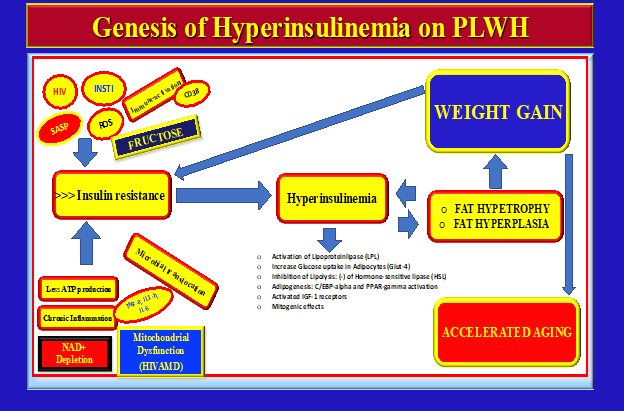
It is well known that the first event that cause hyperinsulinemia is increased insulin resistance. The compensatory hypersecretion of insulin by the pancreas in response to insulin resistance will increase the size of the adipocytes since insulin is lipogenic and will promote the accumulation of triglycerides within the fat cells.18 Fat hypertrophy can be seen as a “compensatory response” due to the excess of nutrients and insulin that other tissues can’t utilize due to resistance. Eventually, once the adipose cells cant expand anymore in size fat hyperplasia may ensue in response to hyperinsulinemia. Both hypertrophy and hyperplasia can be seen during hyperinsulinemia. Of note, fat hypertrophy has been associated more to metabolic complications and cardiovascular disease.17
On Figure 1 we can see an hypothesis on how weight gain on PLWH may be explained in the context of insulin resistance and hyperinsulinemia. Of note, insulin resistance is the original molecular event, caused by many factors (viral and non-viral dependent) all interconnected.

HIV-Associated-Mitochondrial-Dysfunction (HIVAMD): A Distinctive Feature of HIV-Associated Aging
Even though the genesis of weight gain is complex and likely multifactorial mitochondrial dysfunction may play an important and specific role. Mitochondrial dysfunction during lipoatrophy has been extensively documented in the past but its role on fat hypertrophy on the current ART era needs to be further elucidated.19,20 There are some reports however that link integrase strand transfer inhibitors (INSTIs) use and Visceral Adipose Tissue (VAT) hypertrophy with mitochondrial dysfunction, increased adipogenesis , and fat fibrosis17 along with progressive decrease of adiponectin and increase of insulin resistance.
Aging in the general population has been linked to age-related progressive mitochondrial dysfunction (MD) which has become as one of the recognized “Hallmarks of Aging”.21–24 Our group adopted the term HIVAMD to describe MD specifically on PLWH as it may have particular distinctive characteristics and contribution to the accelerated aging process. On the other hand the overconsumption of Ultra-processed foods (UPFs), specially excess of Fructose, has also being linked to metabolic syndrome ,inflammation, microbial translocation, MD, and fatty liver,25–30 hence, an unhealthy diet may also accelerate the aging process of PLWH and may be contributing to HIVAMD and weight gain.
“…..Little is known about the possible mechanisms that cause HIVAMD on PLWH, if there is any link between HIVAMD and metabolic complications (weight gain and metabolic syndrome), and if UPFs may be the “igniter” or “starter” that accelerates that process…”
The objective of this review is to propose a mechanism that may link insulin resistance, hyperinsulinemia, HIVAMD, microbial translocation on the GI tract, metabolic complications (mainly weight gain), and the possible contribution of the consumption of UPFs with the ultimate goal of defining future targets for prospective clinical trials.
1) Mechanisms Linking HIVAMD to Insulin resistance, Hyperinsulinemia, and Weight Gain
HIVAMD on PLWH can cause a deficit in energy production with decreased energy expenditure due to impaired OXPHOS (oxidative phosphorylation) with detrimental consequences for human metabolic health. HIVAMD has been linked to metabolic complications like insulin resistance and type 2 diabetes in PLWH.31
The molecular links between HIVAMD with insulin resistance and metabolic syndrome remain unknown but the following points are some theoretical speculations32:
-
Hypothesis of the serine phosphorylation33 of IRS1/2 (insulin receptor): the phosphorylation of the insulin receptor (IR) mediated by cellular kinases can interfere with the insulin signaling pathway, hence, creating insulin resistance. Of note, the activation of cellular serine kinases is mediated by ROS which can be generated during mitochondrial dysfunction due to increased oxidative stress.
-
Hypothesis of NAD+ depletion with decrease activation of Sirtuis: NAD+ depletion may be one of the triggers of HIVAMD. It is well known that NAD+ is one the main activators of Sirtuins. Under normal conditions mitochondrial Sirtuins (3 to 5) can protect against mitochondrial generation of ROS through de-acetylation, hence, decreasing the activation of serine kinases allowing the insulin receptor to deploy its full function.33 Because of the above, NAD+ depletion with lack of Sirtuins activation can potentially be responsible for insulin resistance and metabolic consequences due to unopposed phosphorylation of cellular kinases (see above).
-
The decrease in the effectiveness of OXPHOS with less ATP production during HIVAMD can potentially disrupt the insulin signaling pathways in insulin-sensitive tissues. Excessive ROS production on HIVAMD in addition to activate the serine kinases can disrupt other molecules of the insulin metabolic pathway as well.34,35
-
On pancreatic beta cells ATP is essential for insulin secretion and functioning34 once the cell senses incoming glucose molecules. The decrease on OXPHOS during HIVAMD may disturb this pancreatic beta cells stimulus since less ATP is produced.
-
Excessive ROS production on HIVAMD may affect the opening of calcium channels necessary for insulin release in pancreatic beta cells.
-
Oxidative stress can damage cellular components of insulin sensitive tissues like adipocyte tissue and muscle reducing the responsiveness to insulin and promoting hyperglycemia and insulin resistance. ROS can also impair the insulin-mediated glucose uptake on insulin-sensitive tissues leading to insulin resistance.36
-
HIVAMD could alter the balance between fission and fusion (altered mitochondrial dynamics) which can alter insulin sensitivity.32 It has been shown that excessive mitochondrial fission (division and segregation of mitochondria) can cause insulin resistance35 mainly due to increased oxidative stress.
-
Damaged mitochondria can impair fatty acid beta oxidation with accumulation of cellular lipids in non-adipose tissue like skeletal muscle and liver (ceramides and diacylglycerols) causing insulin resistance through interruption of insulin pathways and impaired glucose uptake.34,37
-
HIVAMD could trigger inflammatory cellular pathways and a stress response, like the unfolded protein response (UPR) and endoplasmic reticulum (ER) stress both of which can cause insulin resistance.38
The links between anti-retroviral therapy (ART) with weight gain remain unknown but possible explanations are that patients on INSTI may have increased fibrosis, increased adipocyte size (adipocyte hypertrophy), increased adipogenic markers expression (like PPARG and CEPBA), reduce expression of brown and beige fat genes, and insulin resistance.17
There could be a reciprocal relationship between HIVAMD and metabolic complications:

“……Is HIVAMD the genesis of the metabolic complications observed on well controlled HIV patients on ART or is it it’s consequence?…..”
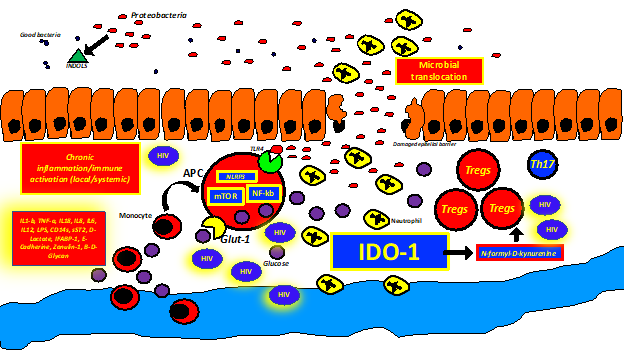
On Figure 2 we can see a proposed integrative mechanism for weight gain on PLWH on which the consumption of UPFs (see section below) may play a very important role:

2) The Role of Ultra-processed Foods (UPFs) in HIVAMD and Metabolic Complications
HIVAMD may be caused not only by the HIV itself or its treatment but because of an unhealthy diet rich in UPFs, especially Fructose.39
"….some PLWH suffer from socioeconomic disparities having access only to highly processed foods with poor nutritional value, high caloric intake, and
detrimental metabolic consequences instead of having access to more healthy, whole foods,40…."
Excessive fructose consumption has been associated to fatty liver, hepatic insulin resistance, diabetes, obesity, and dyslipidemia.39 The increase in the consumption of fructose during the last 50-70 years have been exponential. Ninety percent of the metabolism of fructose happens in the liver. There is a fundamental difference between the metabolism of glucose and fructose. After being phosphorylated by the enzyme Fructokinase and thereafter by the Aldolase b fructose gives rise to 2 trioses: Di-hydroxyacetone-P and Glyceraldehyde-3P (See Figure 3). When there is also available glucose as the source of energy the trioses are drifted to the DE NOVO LIPOGENESIS PATHWAY which are either shipped within the VLDL or starts the process of liver inflammation of fatty liver due to tissue accumulation (Figure 3). Another byproduct by the trioses is METHYLGLYOXAL (MGO) which cause mitochondrial dysfunction and damages proteins by glycation ( 72-74-76). During the above enzymatic reactions an excess of ATP is consumed with intracellular ATP depletion (because fructokinase consumes ATP to phosphorylate the fructose). The resultant accumulation of AMP drives the formation of URIC ACID (data shows that fructose consumption correlates with hyperuricemia and hypertension). In the context of fructose overconsumption the cell senses a “low energy status” (due to ATP depletion) which activates AMPK. The Fructokinase enzyme is poorly regulated which means that most of the fructose will be phosphorylated as far as it keeps coming in, consuming most of the ATP.
“…..Paradoxically, fructose overconsumption with subsequent ATP depletion (with the resultant AMP accumulation) activates AMPK (molecular sensor of “low energy” cellular status) stimulating glucose transport, glycolysis, beta-oxidation, inhibiting mTOR, activating mitochondrial biogenesis (mitochondria production), and autophagy in order to PRODUCE energy (catabolic pathways)27–30,39….”
However during chronic fructose overconsumption the rate of glucose transport is diminished due to insulin resistance, there is de novo lipogenesis, and increased cholesterol synthesis leading to metabolic syndrome. The reason behind is that MGO causes allosteric modifications of AMPK rendering it inactive and not activated by AMP.


“….Methylglyoxal (MGO) can contribute to HIVAMD due to advanced glycation of mitochondrial structural proteins, lipids, and mDNA causing an increase of ROS and inhibition of manganese superoxide dismutase (mnSOD), one of the main anti-oxidants. Also, MGO inhibits the protein complex III of the electron transfer chain (ETC) decreasing the production of ATP. MGO has been associated to other hallmarks of aging like systemic inflammation, loss of proteostasis, genomic instability, and promotion of cellular senescence41….”
3) Microbial Translocation and Gut Health in PLWH in the context of Fructose Overconsumption and HIVAMD
There is existing evidence that microbial translocation in a dysfunctional and structurally abnormal GI mucosal barrier is of paramount importance on HIV pathogenesis.42–50 Epithelial damage and microbial translocation triggers chronic inflammation and immune activation and has been reviewed in detail elsewhere.51–56 In our recent review we explored this concept more in detail (https://doi.org/10.59541/001c.84063)(see Figure 4).

It has been shown in mice that fructose consumption produce dysbiosis, leaky gut, and liver inflammation and fibrosis30 through decrease in the levels of tight junction proteins (zonula occludens-1, occluding, claudin-1, and claudin-4), adherent junction proteins, and desmosomes.
“…Fructose overconsumption may worsen the already existent microbial translocation and dysbiosis at the intestinal mucosa level on PLWH exacerbating the functional and structural damage of the tight junction proteins contributing even more to local and systemic inflammation30….”
HIV associated dysbiosis can potentially cause HIVAMD and metabolic complications (including weight gain) through the following mechanisms:
-
Activation of TLR4 due to microbial translocation through products like LPS with resultant immune activation and systemic inflammation and generation of oxidative stress which is detrimental for mitochondrial function (see prior sections).
-
Microbial translocation with activation of the receptor CD14 promotes visceral adipose fat (VAT) inflammation through activation of M1 macrophages (pro-inflammatory phenotype) or “Metabolic Switch” increasing the secretion of IL-6, TNF, and other cytokines.17
-
Changes on the microbiota on PLWH may have not only detrimental effects on the mitochondrial function but metabolic consequences as well, probably mediated through systemic inflammation e immune activation with promotion of oxidative stress. Of note, a microbiome with predominance of Proteobacteria and Prevotella with less Bacteroides and Firmicutes may be highly pro-inflammatory and predispose to weight gain.51,55–58
-
Microbial translocation could cause endothelial dysfunction with impairment on the delivery of O2 to several tissues on which the mitochondrial function may be affected due to decreased OXPHOS and switch to pro-inflammatory and glycolytic pathways.
-
Significant decrease of the short chain fatty acids during HIV-associated dysbiosis may potentially affect mitochondrial function, specially of intestinal epithelial cells.58
-
Some “leaked” microbial products like LPS or 1-3-D-Beta glycans may potentially cause mitochondrial damage directly on distant tissues with subsequent insulin resistance and other metabolic consequences.
4) Omega-6/Omega-3 Ratio and Mitochondrial Function
There is evidence that the excess of Omega 6 fatty acids relative to Omega 3 fatty acids on Western diets can cause mitochondrial dysfunction and systemic inflammation. Specifically, oxidized linoleic acid can induce mitochondrial dysfunction, apoptosis, and NLRP3 activation in mice.59,60
“….Diets with an Omega-6/Omega-3 ratio of 30:1 may trigger inflammation. Diets with an Omega6/Omega3 ratio of 3:1 or 1:1 may either prevent or reduce inflammation respectively….”
Screening and Diagnosis
The distinction between obesity and fat hypertrophy can be challenging. In general fat hypertrophy is distributed mainly on visceral adipose tissue (VAT) or truncal areas. As mentioned above the BMI may underestimate the fat mass percentage due to concomitant muscle mass loss but it should be measured at least yearly on PLWH. There are other more efficient measurements that can measure VAT:
-
Waist circumference
-
Waist to hip ratio
-
A DEXA scan is always preferred if it is available
Considering that insulin resistance and hyperinsulinemia may be the first two molecular events early during the course of the metabolic complications of PLWH on ART the following blood tests may be indicated early in the course and as a baseline before starting INSTI or TAF:
-
Homeostatic Model Assessment for Insulin Resistance (HOMA-IR)
-
Isolated fasting insulin levels
Baseline fasting glucose levels and hemoglobin A1c may not reflect the early changes on the metabolic profile. For example, the fasting glucose levels may be normal due to compensatory hyperinsulinemia secondary to insulin resistance. Hemoglobin A1c may be a late marker of metabolic complications since it will show glycosylation of proteins due to hyperglycemia during the preceding 3 months.
Conclusions and Future Perspectives
PLWH are suffering from a significant number of age-associated diseases at an accelerated rate otherwise usually seen in older HIV(-) populations. HIVAMD may be highly associated with this pattern of accelerated aging on which metabolic syndrome, insulin resistance, fatty liver and weight gain are becoming a threat not only to the lifespan but the healthspan of PLWH. Here we proposed a mechanism for which HIVAMD is directly linked to aging and its metabolic consequences, with especial emphasis on the deleterious consequences of the consumption of UPFs as an “accelerator” of an existent metabolic problem. UPFs also can exacerbate microbial translocation which is a known contributor of systemic inflammation and immune activation on PLWH. Prospective, pragmatic, easy to perform trials are needed to assess the response of dietary interventions and nutritional supplements of HIVAMD and it’s metabolic complications. Pragmatic research should be started at community hospitals, non-profit organizations, and community centers with well-funded resources from governmental and non-governmental organizations.
Accessible lifestyle changes like Intermittent fasting (InF) or its variation “early time restrictive feeding (eTRF)” may be effective tools in order to revert the hyperinsulinemia, improve the insulin sensitivity, inhibit mTOR, promote autophagy, increase lipolysis, and improve mitochondrial function.61–64 Intermittent fasting studies should be performed only on medically supervised, well-controlled prospective clinical trials. Other pharmacological measures like Semaglutide, Liraglutide, Metformin, Temsarolin need to be further explored in PLWH with the goal of decreasing VAT and cardio-metabolic complications.