Introduction
SARS-CoV-2 is an enveloped, positive-sense, single-stranded RNA betacoronavirus first identified in a report of cases of acute respiratory illness in Wuhan Hubei Province, China in December 2019.1 The virus spread widely and rapidly and quickly became a world-wide public health emergency. By June 2020 over 6 million cases and nearly 400,000 deaths were reported world-wide.2 Vaccines to prevent COVID-19 infection and severe disease were first approved for emergency use in the United States (US) in December 2020. Numerous early phase vaccine trials beginning in mid-2020 rapidly enrolled subjects resulting in Emergency Use Authorizations in the US for vaccines manufactured by Pfizer, Moderna, Janssen (Johnson and Johnson), and Novavax.
Starting in mid-2020 and lasting to 2023, Norton Research Institute (i.e., Norton Healthcare Louisville, KY), the University of Kentucky and Baptist Health Lexington formed a collective Kentucky unit to study the Janssen Ad26.COV2.S COVID-19 vaccine. The Ad26.COV2.S vaccine is a recombinant, replication-incompetent adenovirus serotype 26 vector which encodes a full-length SARS-CoV-2 spike-protein.3 It was during this time, according to the data published by the Kentucky Department for Public Health which utilized the population values from the 2019 US Census Bureau Estimates, COVID-19 infections affected Kentucky and the virus underwent multiple mutations including two periods when Kentucky experienced a substantially higher incidence rate. The COVID-19 Omicron variant surge in January 2022 led to an overall daily incidence rate as high as 237.01 per 100 thousand population, and 42.88 per 100 thousand population during the Omicron subvariant surge that occurred between June-July 2022.4
The Kentucky unit became a high enrolling site for Janssen clinical COVID-19 vaccine trials including enrollment in the phase 3 trial “A Study of Ad26.COV2.S for the prevention of SARS-CoV-2 Mediated COVID-19 in Adult Participants (ENSEMBLE-1)”.3 This phase 3 trial evaluated the safety and efficacy of the Ad26.COV2.S vaccine in preventing or lessening the severity of molecularly confirmed severe acute respiratory SARS-CoV-2 compared to placebo in participants 18 years and older. During the latter part of the ENSEMBLE-1 trial, the US FDA (Food and Drug Administration) conducted an inspection of the ENSEMBLE-1 Kentucky unit and reported that the unit followed the protocol without any objectionable deviations.
In addition, the University of Kentucky enrolled participants in 2 other Ad26.COV2.S vaccine trials, ENSEMBLE-2 and AMPIFY.5,6 Data from these three trials allowed us to compare the efficacy of a prime and single boost with the Ad26.COV2.S vaccine to any other combination of prime and boost (single or multiple boosts) vaccinations that included not only Ad26.CVO2.S but other available COVID-19 vaccines available during this period, mainly the mRNA vaccines from Pfizer and Moderna.
Methods
For all three trials, subjects were 18 years or older, in good health (neither pregnant nor planning to be), without an abnormal immune conditions or cancer (except for some skin cancers or cervical cancer in situ), and without chronic active hepatitis B or C. Subjects with HIV and CD4 count >300 cells/uL and HIV viral load< 50vp/mL were included. The University of Kentucky IRB numbers were 61673 (ENSEMBLE-1), 64399 (ENSEMBLE-2) and 70658 (AMPLIFY).
Enrollment for ENSEMBLE-1 began in October 2020 with the last follow-up completed in January 2023. At the conclusion of the double-blind phase, participants were unblinded at Month 6 after their prime vaccination; those who originally received placebo were offered a single dose of Ad26.COV2.S. The study continued as open-label and all participants were offered an Ad26.COV2.S booster dose at their Year 1 visit. Those participants who received mRNA COVID-19 vaccines outside of the trial were allowed to remain in the trial. Enrollment in the two additional Janssen Ad26.COV2.S trials are included in the results. Both trials began after the start of the ENSEMBLE-1 trial. ENSEMBLE-2 compared a single Ad26.COV2.S dose to a single Ad26.COV2.S dose followed by an Ad26.COV2.S booster 6 weeks later. AMPLIFY offered an Ad26.COV2.S booster to those who previously received either a Pfizer mRNA vaccine prime or an Ad26.COV2.S prime. Subjects were included in this analysis who could be followed through July 2022 or up to their initial COVID-19 infection. Although most of the data analysis is descriptive, Chi-Square comparisons were performed between the two groups. Group 1 includes those who received only a prime and single booster with the Ad26.COV2.S. Group 2 includes those who received any other combination of prime and booster(s).
Results
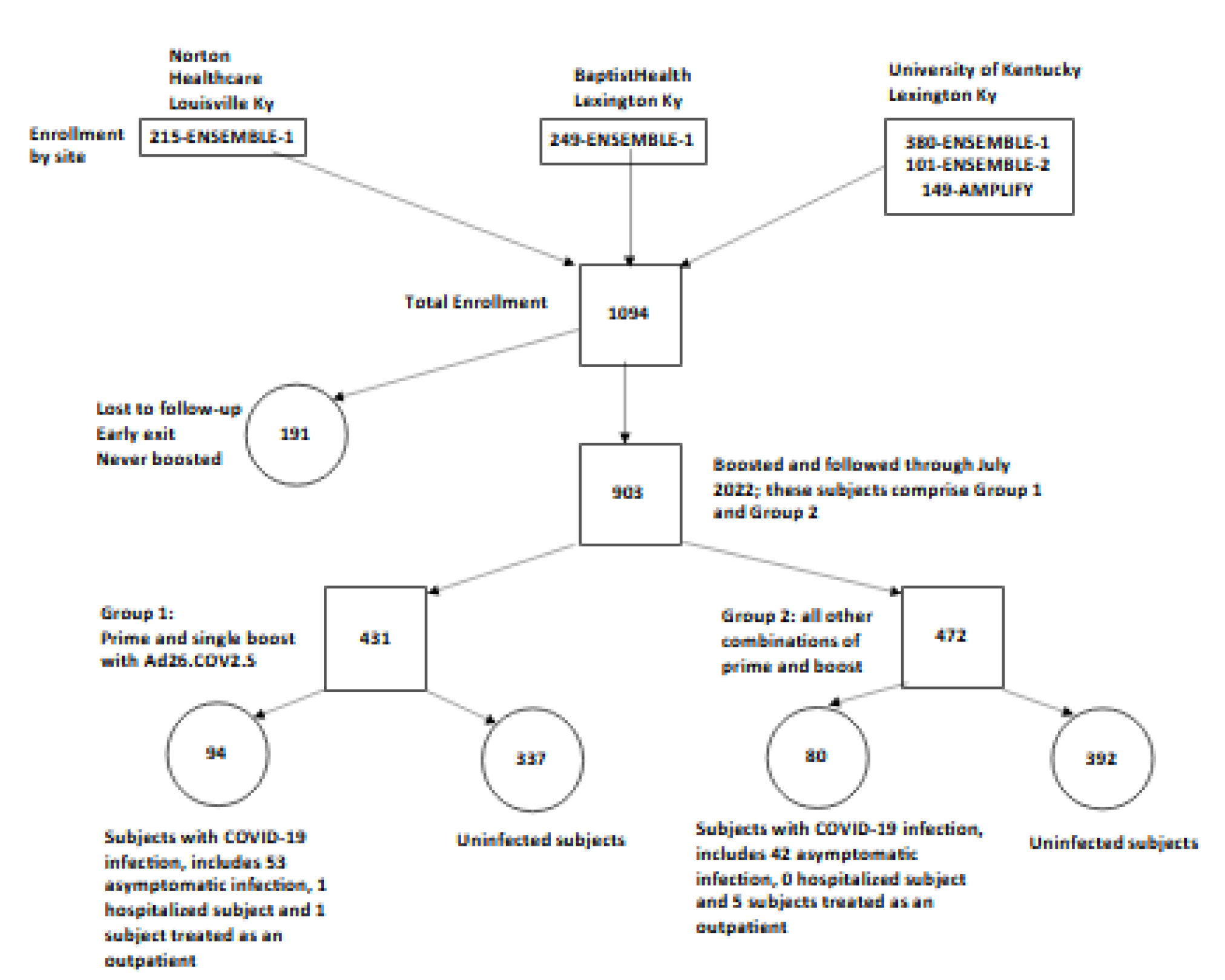
The Kentucky unit enrolled 1,094 subjects: 844 subjects in ENSEMBLE-1, 101 subjects in ENSEMBLE-2, and 149 subjects in AMPLIFY. Overall, the mean age was 53 years and mean BMI was 28; 45% of participants were male. 191 subjects were not included in the analysis, 160 subjects in ENSEMBLE-1, 29 in ENSEMBLE-2 and 2 in AMPLIFY. These participants either had a COVID-19 infection prior to their first booster, did not receive a booster, or exited the trials before they could be evaluated for vaccine efficacy through July 2022 (Figure-1).

903 of the 1,094 enrolled subjects (83%) were nucleocapsid seronegative at the time of their first booster which could have been an Ad26.COV2.S or a mRNA vaccine, were not known to have had COVID-19 and could be evaluated for vaccine efficacy through July 2022. This included 175 participants (19%) vaccinated with mRNA vaccines only. The majority of all first boosters (96%) were given prior to 2022.
Participants evaluated for vaccine efficacy were placed in one of two groups as described in the Methods: 431 (48%) received only a prime and single boost with Ad26.COV2.S (Group 1) and 472 (52%) received any other combination of prime and boost(s) vaccines (Group 2). Group 1 consisted of 53% male, average age of 54 years, average BMI of 29.5 and 10 diabetics; Group 2 had 44% males, average age of 48 years, average BMI of 29.8, seven diabetics and included 22% primed with an mRNA vaccine (either BNT162b2 (Pfizer-BioNTech) or mRNA-1273 (Moderna)) and boosted once with Ad26.COV2.S, 14% primed with Ad26.COV2.S and boosted with an mRNA vaccine, 37% primed and boosted once with an mRNA vaccine, and 27% primed and boosted multiple times with various combinations of Ad26.COV2.S and mRNA vaccines.
Between January 2021 through July 2022, a time when there was a high incidence rate of COVID-19 infections and death in the state of Kentucky, there were 174 breakthrough COVID-19 infections. 43 of which were in participants aged 70 years or older. 95 of the 174 (55%) were considered asymptomatic (53 (56%) of these participants were in Group 1).
During January 2022 there was a surge in COVID-19 Omicron infections. 104 of the 174 COVID-19 breakthrough infections occurred during this surge and included 58 in Group 1 and 46 in Group 2 (P>.05). Only 2 cases in each group had been boosted more than 6 months earlier. None of the 104 cases were hospitalized. One Group 1 subject and five Group 2 subjects were treated with Nirmatrelvir-Ritonavir in an outpatient setting.
During June-July 2022, Kentucky experienced another COVID-19 surge due to Omicron BA.1, BA.2, and BA.5 subvariants. As a result, there were an additional 70 breakthrough infections that included 36 in Group 1 and 34 in Group 2. Of the 36 who received only Ad26.COV2.S, 32 of the 36 received their only booster more than six months earlier. Only one of six individuals treated with Nirmatrelvir-Ritonavir was in Group 1.
Overall, the efficacy of the Ad26.COV2.S vaccine as a prime and boost series (94 infections, Group 1) was not significantly different (P>.05) from that of any other series of vaccinations (80 infections, Group 2). During the study period, just one subject was hospitalized for a COVID-19 infection. The subject was a 75-year-old male with type 2 diabetes who received a prime and single boost of Ad26.COV2.S. He was hospitalized in November 2021, 3 months after his booster, and recovered without requiring a ventilator. There were no instances of vaccine-related serious adverse events such as vaccine induced thrombosis and thrombocytopenia, post vaccination Guillain-Barre syndrome or deaths due to SARS-Cov-2 in the 1094 study participants.
Discussion
From January 2021 to July 31, 2022 the prime and single boost combination of Ad26.COV2.S vaccine (Group 1) appeared to protect immunocompetent adult study subjects from severe infection and hospitalization for at least 6 months as well as any other boosted regimen (Group 2). A similar result was reported in a study from South Africa that compared Ad26.COV2.S prime and boost to BNT162b2 prime and boost during an Omicron surge.7 In addition, the Group 1 data appear consistent with previously published safety results, such as those from a phase 1-2a multicenter, randomized, placebo controlled trial which reported findings that support an acceptable safety and reactogenicity profile for Ad26.COV2.S.8
Although this report does not include the results of a single Ad26.COV2.S vaccination as booster vaccinations were offered to all subjects, it is important to know that the ENSEMBLE-1 trial found a single-dose of Ad26.COV2.S to be 77% effective against severe-critical COVID-19 disease with onset at least 14 days after administration and 85% effective against severe-critical COVID-19 disease with onset at least 28 days after administration.9 One might hypothesize that the additional Ad26.COV2.S booster would improve durability and benefit those with weakened immune systems as well as the elderly.
Unfortunately for Janssen, Ad26.COV2.S was associated with the following major concerns that lessened its appeal to the US public. (1) Although given US Emergency Utilization Authority (EUA) on February 27, 2021, on March 13, 2021 the US FDA and the CDC (Centers for Disease Control and Prevention) paused the use of Ad26.COV2.S over concern for an increased association with an extremely rare clotting disorder “cerebral venous sinus thrombosis (CVST)”. At that time CVST had been reported to have an increased association with another adenoviral vector COVID-19 vaccine manufactured by AstraZeneca (a vaccine never distributed or approved in the United States); CVST had also been associated with mRNA COVID-19 vaccines but to a lesser extent.10,11 The pause lasted 11 days but the concerns about this potentially lethal serious adverse event continued. In December of 2021, the CDC recommended that the mRNA vaccines be used as the preferred vaccines against COVID-19 and in May of 2022 the US FDA limited the use of Ad26.COV2.S to those 18 years and older who were unwilling or unable to get an alternative COVID-19 vaccine. Nearly 40% of the Ad26.COV2.S supplied to the United States went unused. (2) Ad26.COV2.S production in the United States was mired in a perplexing situation where tens of millions of Ad26.COV2.S doses had to be destroyed due to quality control issues and contamination at an Emergent BioSolutions’s facility contracted to manufacture the vaccine in the US. (3) In May of 2023, the World Health Organization (WHO) reassessed the COVID-19 vaccine formulations and requested a new formulation to address the virus’s continuing mutations and variations in its circulating strains. In June 2023, the US made the same request. In a letter to the US FDA dated May 22, 2023, Janssen informed the US FDA that due to lack of demand for its Ad26.COV2.S vaccine and that all current lots had expired, the company would not update the Ad26.COV2.S formulation and withdraw it from production. Indeed, Janssen made similar decisions with other vaccines being developed (i.e., Respiratory Syncytial Virus (RSV)) as well as a company overhaul of its product development strategy.
Nevertheless, while Ad26.COV2.S was being studied in the US, it was also being distributed world-wide. Attributes contributing to the efficacy of Ad26.COV2.S included a broader T-Cell (e.g., cellular immunity) response than other COVID-19 vaccines including mRNA vaccines, rising antibody levels over time as the humeral immune response was more durable than mRNA vaccines, lack of significant thrombosis with thrombocytopenia syndrome with a second or additional doses and a significant increase in antibody responses with a heterologous vaccine schedule that included both Ad26.COV2.S and mRNA vaccinations over that of a homogeneous vaccination schedule.12–15 In addition, the Ad26.COV2.S vaccine had favorable storage conditions (requiring only -20 °C freezer storage whereas mRNA vaccines required -80°C for storage) that provided opportunities to expand access to COVID-19 vaccination across the globe. One might postulate that reducing the dose of antigen in Ad26.COV2.S and adding boosters might have had major safety advantages over the original formulation. According to the Centers for Disease Control and Prevention’s COVID Data Tracker, the Ad26.COV2.S vaccine had been administered across 106 countries representing an ethnically and geographically diverse population with myriad SARS-CoV-2 variants.16 An estimated 7% of Kentucky’s population received the Janssen vaccine as their first dose.4
As previously mentioned, this trial was conducted during two periods when Kentucky experienced a substantially higher incidence rate, January 2022 and June-July 2022.4 High incidence rates have been associated with decreased vaccine efficacy in the past. However, despite the increased transmission and development of numerous viral variants, the prime and single boost of Ad26.COV2.S appeared to provide consistent protection from infection and severe disease that was not significantly different from any other vaccine regimen used at that time.
Deficiencies that might have an effect on our data analysis included lack of a placebo control Group, an understandable result of rapid data publication of the efficacy of the mRNA vaccines and the continued severity of the pandemic. There also could not be documentation or comparison of adverse events related to vaccinations received outside the studies. No data was collected for 2 populations, pediatrics and immunocompromised subjects. On the other hand, the Kentucky unit demonstrated cooperation between private and public healthcare organizations located in the Louisville and Lexington area, a cooperation that clearly benefited all those vaccinated and followed by the trials.
The results of that effort demonstrated that both a prime and single boost regimens of the Ad26.COV2.S was as effective as any other boosted COVID-19 vaccine regimen. All regimens protected adult study participants from severe-critical COVID-19 infection, including hospitalizations and death for a minimum of 6 months. Our data extends from January 2021 through July 2022 and supports the durability of the Ad26.COV2.S vaccine as a prime and booster during the first 7 months of the SARS-CoV-2 Omicron variant surge.
Acknowledgements
Additional Norton Research Institute leadership and clinical coordinators contributed in making this trial a success including Stephen Wyatt, DMD, MPH; Marti Gardner, MSN, APRN, CCRC; Jennifer Comings, BSN, CCRC; Melissa Velasco, PMHNP-BC; and Leigh Stoffer, BSN, CCRC. This work and publication was supported by the National Center for Advancing Translational Sciences, NIH(UL1TR001998); the content does not represent official views of the NIH. Gratitude is expressed to the many workers at all 3 sites and to the volunteer subjects.