INTRODUCTION
Community-acquired pneumonia (CAP) has traditionally been viewed primarily as an acute infection of the lungs. In this traditional model, only acute clinical outcomes were considered. However, recent research has shifted our view of CAP, emphasizing that in a significant number of patients, CAP extends beyond the lung to affect multiple organ systems.1 We also recognize that a patient with CAP may have negative clinical outcomes that can manifest months or years after the episode of CAP.1 Hence, today we have a new paradigm when evaluating patients with CAP. We look at these patients as having a multisystemic disease producing acute as well as post-acute or chronic sequelae.1 One important long-term consequence is the decreased survival that occurs in patients after an episode of CAP. Several large studies including more than 1,000 patients have documented long-term mortality in patients suffering an episode of CAP.2–8
The National Institute of Health has identified the systemic and long-term consequences of pneumonia as an important area for future research.9 Even though it is clear that a significant number of patients will suffer from long-term mortality after an episode of CAP, the particular subpopulations of patients with CAP that will be affected as well as the subpopulations at high risk for decreased survival are not fully characterized.
Our research team have performed several studies in the city of Louisville evaluating short and long-term outcomes in patients with and without CAP. In this study, we reviewed our prior work with the objective to define the incidence for long-term mortality in special populations of patients hospitalized with CAP.
METHODS
Study design
This was a retrospective study of two study databases from Louisville, Kentucky: the University of Louisville Pneumonia Study (ULPS) database, and the Louisville Veteran Affairs Medical Center (VAMC) long-term mortality study database. The primary manuscripts from these two databases were previously published.10,11
Subjects
In the ULPS database, patients were included if they were hospitalized at one of the nine adult hospitals in Louisville between June 1, 2014 to May 31, 2016. In the Louisville VAMC study database, patients were included if they were hospitalized for any reason at the Louisville Robley Rex Veteran’s Affairs Medical Center between the dates of June 1, 2001 to November 26, 2006.
Long-term Mortality
Long-term mortality was defined as mortality within one year after the time of hospital admission.
General Population and Special Populations
Long-term mortality was evaluated for the general population of hospitalized patients due to CAP as well as the general population of hospitalized patients to a medical ward for medical conditions other than CAP. Long-term mortality was evaluated for the following special populations: 1) patients hospitalized with CAP who reach early clinical stability, defined as clinical stability within three days of hospitalization; 2) Elderly patients hospitalized with CAP, defined as age ≥ 65 years; 3) Patients hospitalized with CAP with a history of COPD; 4) Patients hospitalized with CAP requiring ICU care; 5) Patients hospitalized with CAP who developed a cardiovascular event during hospitalization; and 6) immunocompromised patients hospitalized with CAP.
Immunocompromising conditions
A patient was defined as immunocompromised if they had any of the following: primary immunodeficiency disease, advanced-stage cancer (stage III or IV solid cancer or hematologic cancer, as defined in the supplementary materials), advanced HIV infection (CD4 T-lymphocyte count <200 cells/mL or <14%), solid organ transplantation, hematopoietic stem cell transplantation, cancer chemotherapy, biological immune modulators, corticosteroid therapy with a ≥20-mg dose of prednisone or equivalent daily for at least 14 days prior to hospitalization, or disease-modifying antirheumatic drugs.
Comorbidities
The number of combined comorbidities or comorbidity stacking, was evaluated for the following comorbidities: 1) Neoplastic disease; 2) COPD; 3) Liver disease; 4) Renal disease; 5) Diabetes; 6) Cerebrovascular disease; 7) Coronary artery disease; and 8) Obesity (body mass index ≥ 30).
Level of immune function
Patients hospitalized with CAP were categorized into 4 ordinal groups based on immune function: 1) no immunologic abnormality (patients aged < 65 years with no comorbidity described above), 2) abnormal immune system (patients aged ≥ 65 years and/or patients with comorbidity described above), 3) immunocompromised (exactly one immunocompromising condition or medication, as described above, regardless of age or comorbidity), or severely immunocompromised (more than one immunocompromising condition, as described above).
Statistical analysis
Incidence of long-term mortality was represented as the percentage of the group or subgroup that died within one year after hospitalization. Bar charts were created to visualize mortality incidence among groups.
Geospatial analysis
Long term mortality was evaluated at the census tract level for all adults hospitalized with CAP in the ULPS database, as well as special populations. Choropleth maps were produced to map long term mortality and identify geospatial trends. All maps were created using ArcGIS Pro version 3.2.
RESULTS
Overall long-term mortality and by sub-population
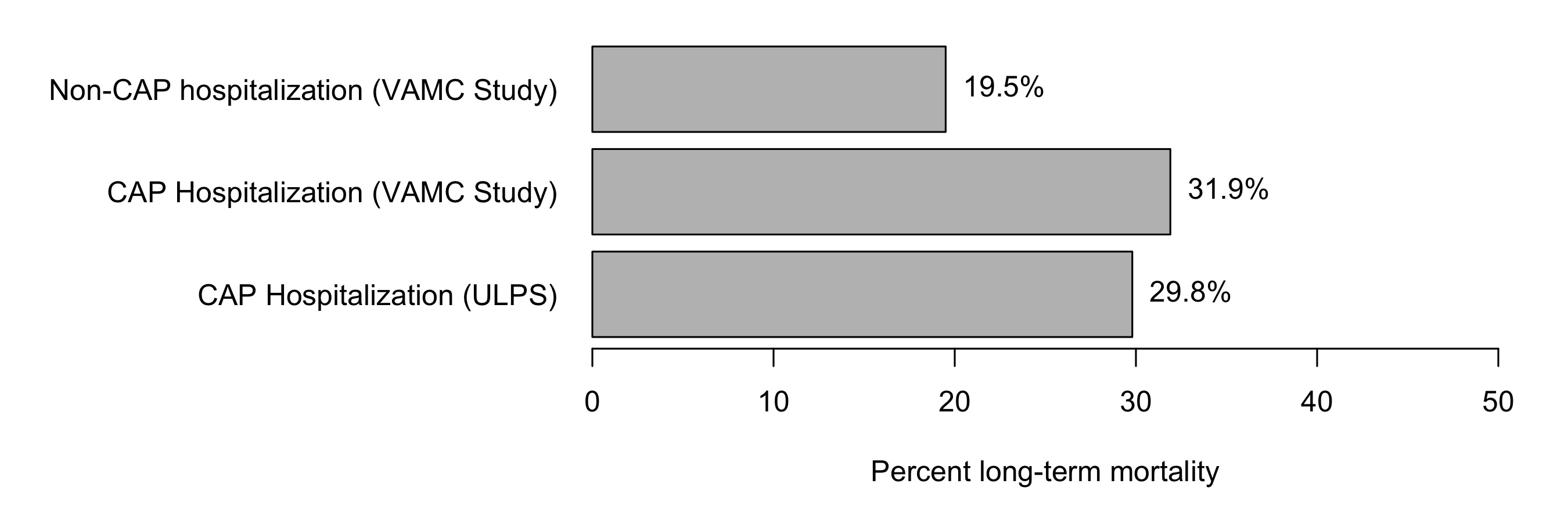
In the VAMC study, a total of 6,347 patients hospitalized without CAP were followed. Long-term mortality for these patients was 19.5%. A total of 624 patients hospitalized with CAP were followed in the VAMC study, with long-term mortality of 31.9%. A total of 7,449 patients hospitalized with CAP were followed for the ULPS, with a long-term mortality of 29.8%. Incidence of long-term mortality by study and cohort are depicted in Figure 1.

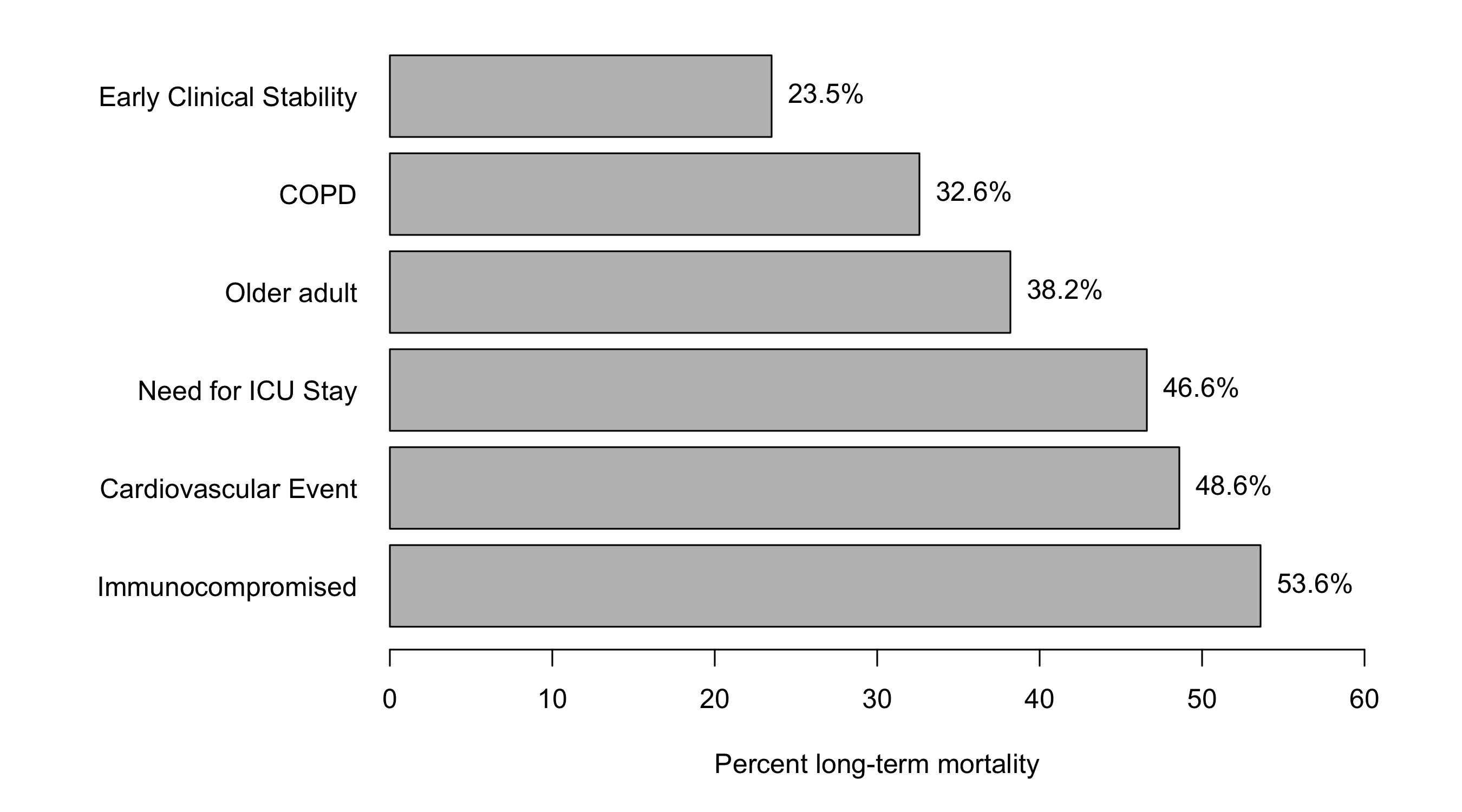
Long-term mortality by subgroup are depicted in Figure 2. The sub-population of patients who reached early clinical stability was experienced lower incidence long-term mortality. Long-term mortality increased depending on risk factors such as COPD, immunocompromising medical conditions or treatments, ICU stay, and advanced age. Additionally, patients who experienced cardiovascular events during hospitalization had an increased long-term mortality.

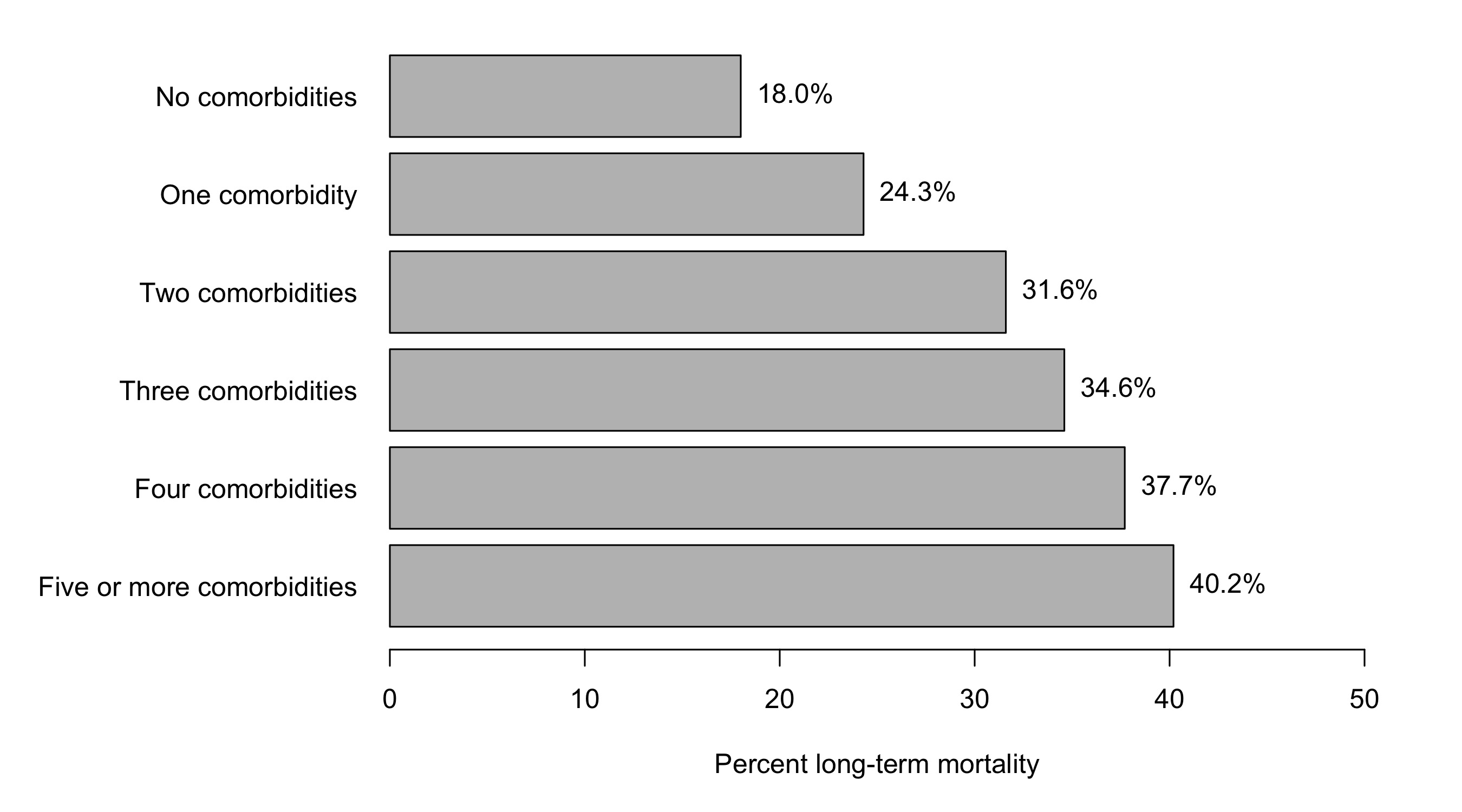
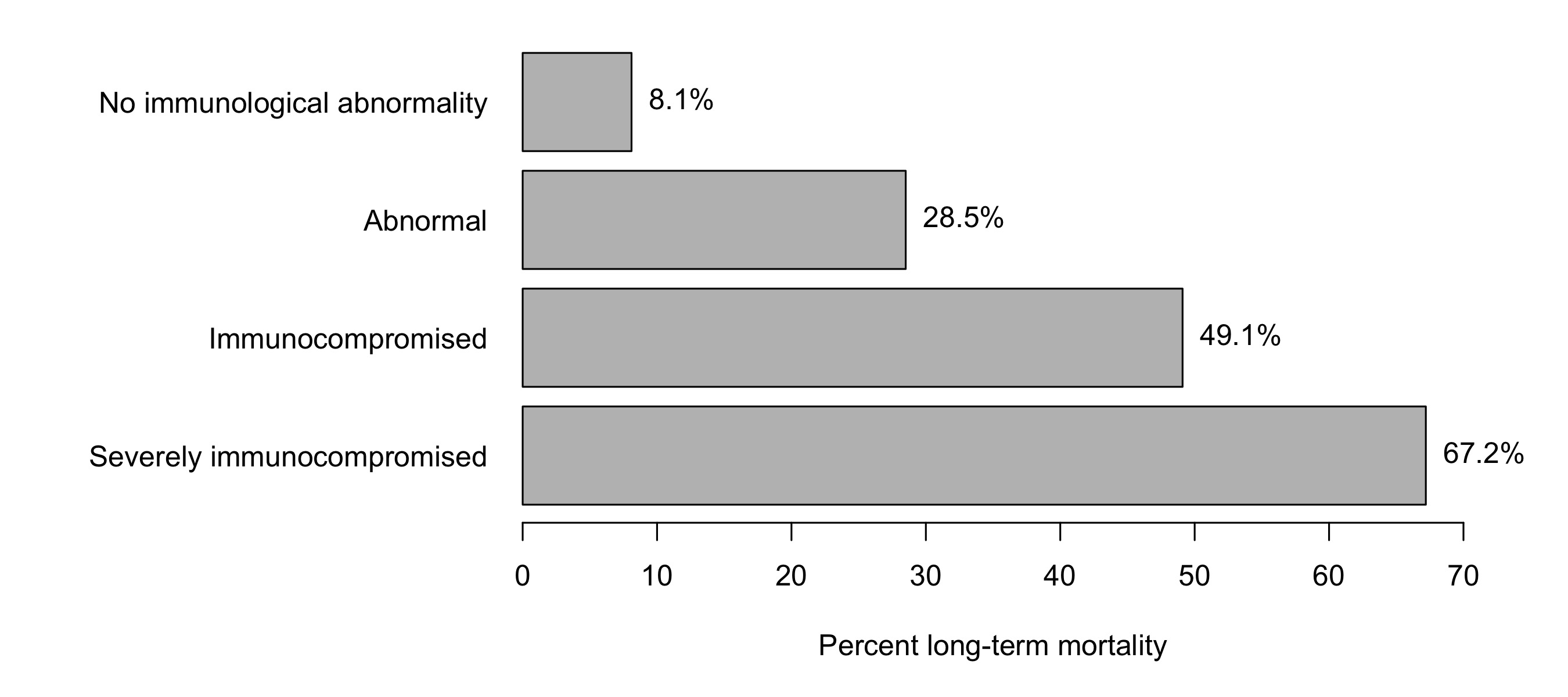
When evaluating comorbidity stacking, incidence of long term mortality increased as the number of comorbidities increased (Figure 3). Additionally, when patients were characterized according to immune function at time of hospitalization, there was increased incidence of long-term mortality in patients characterized as having decreased immune function (Figure 4).


Geospatial analysis
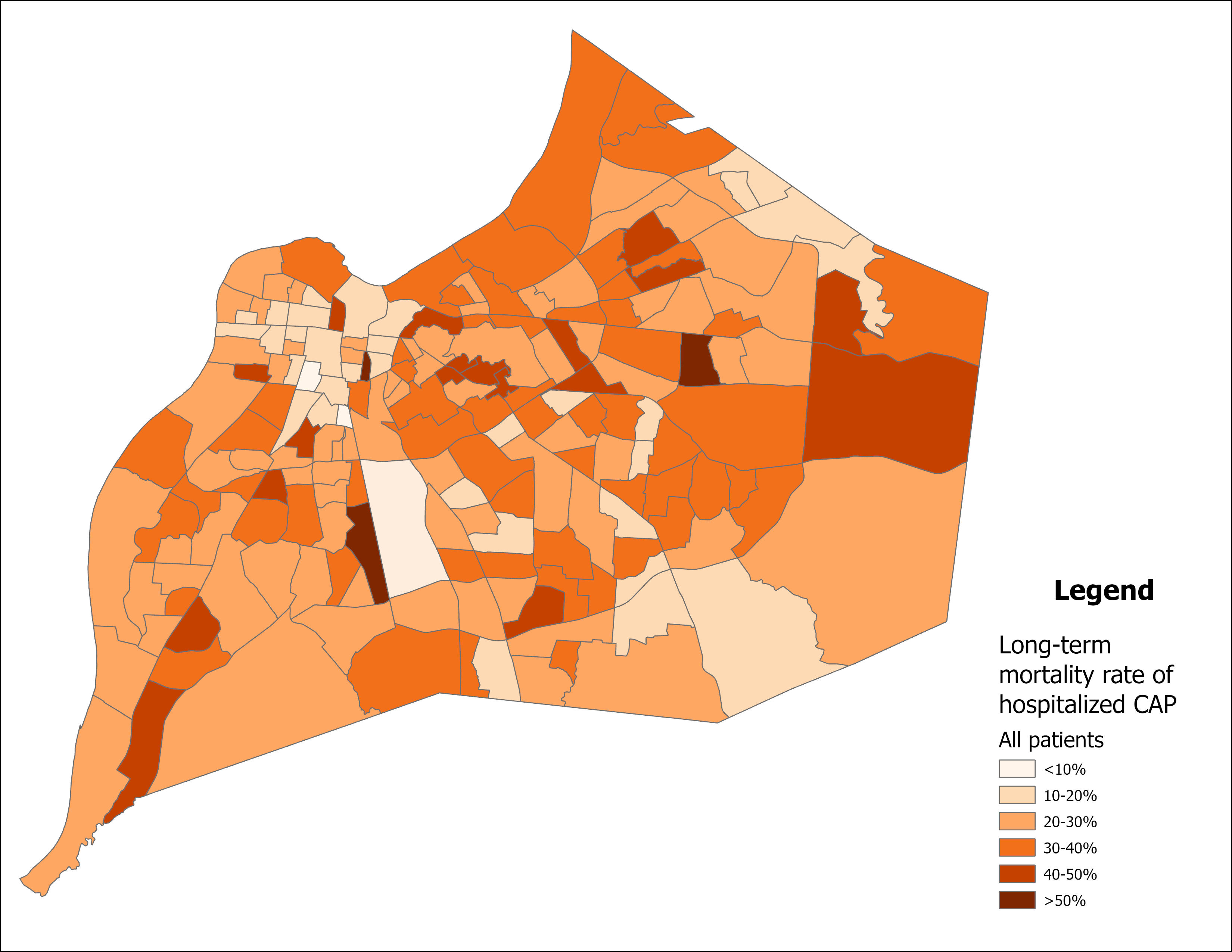
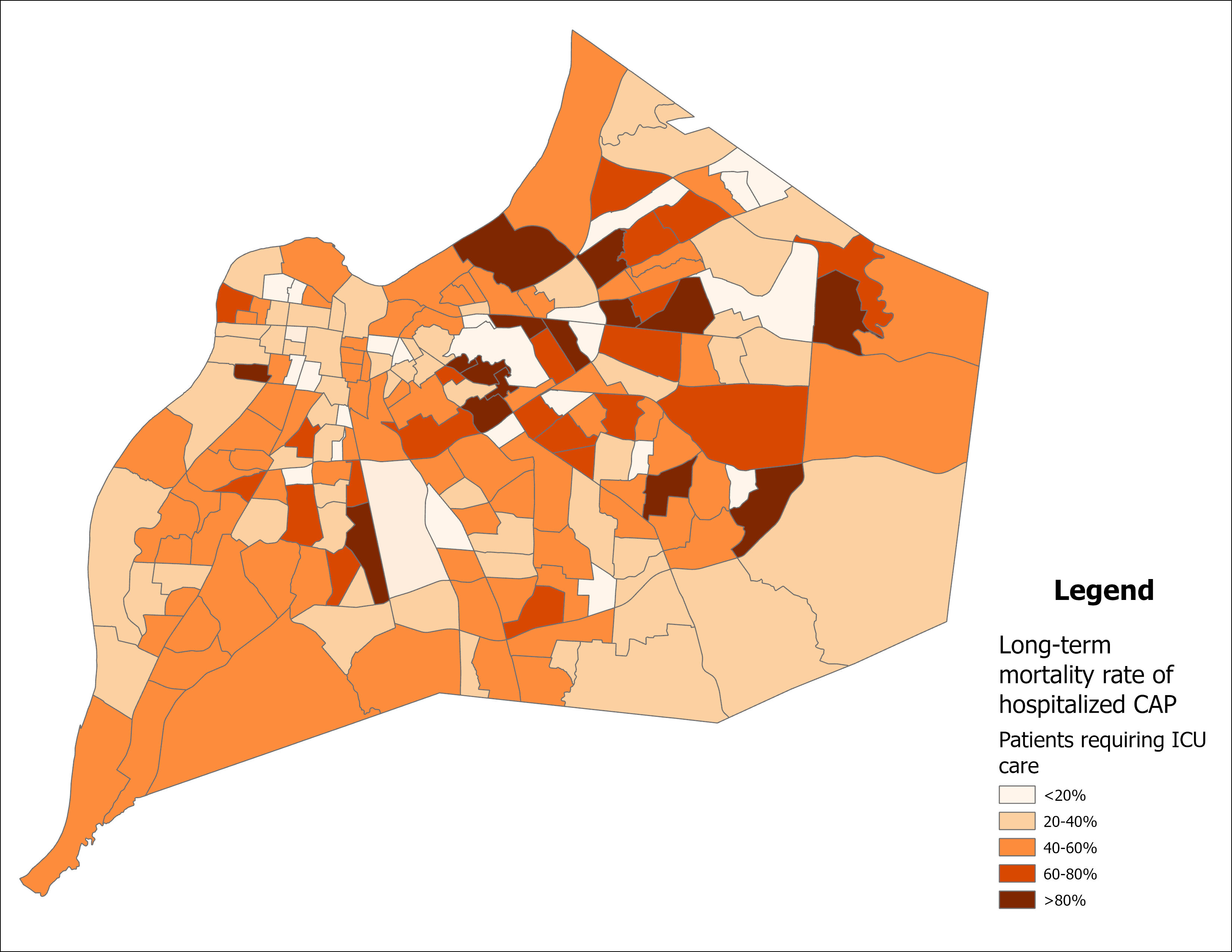
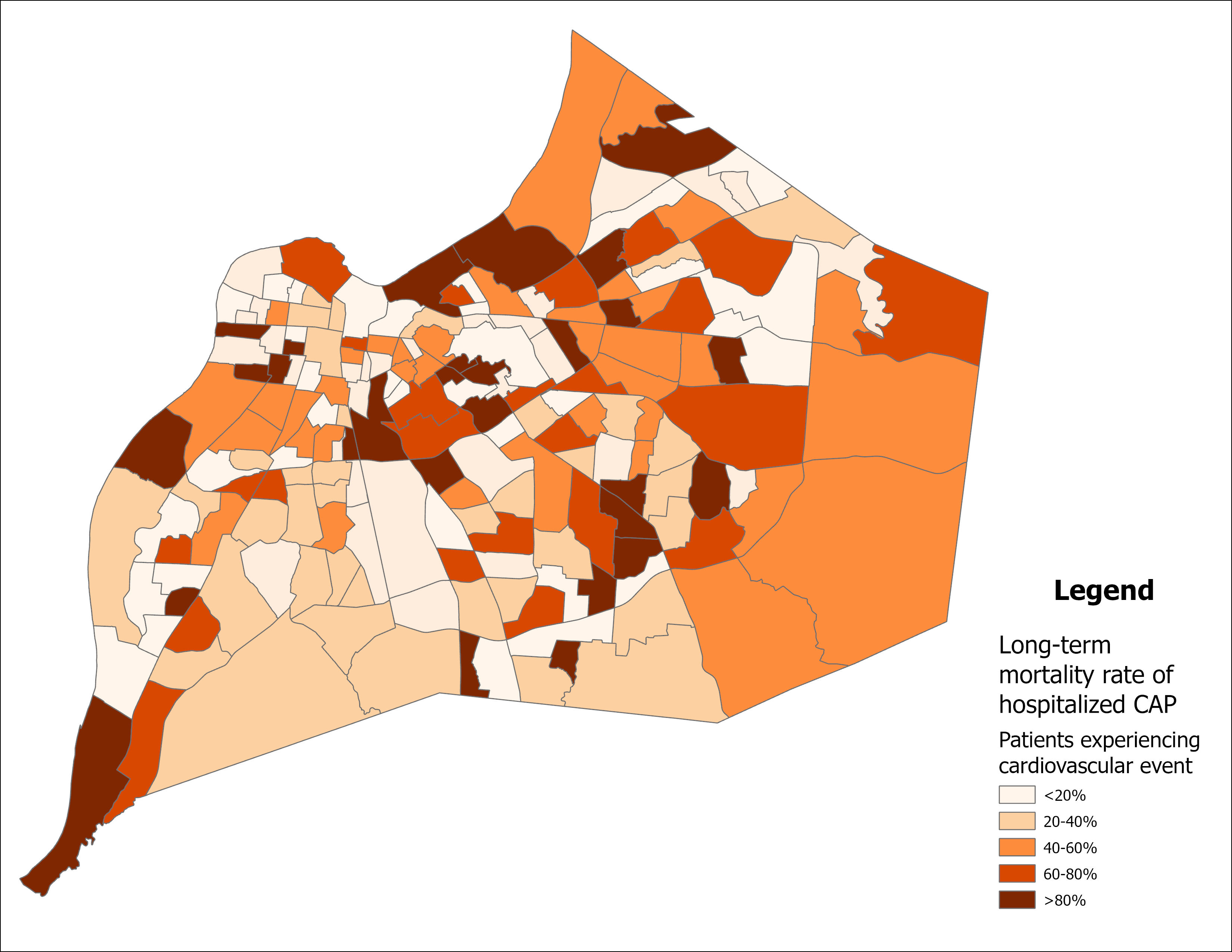
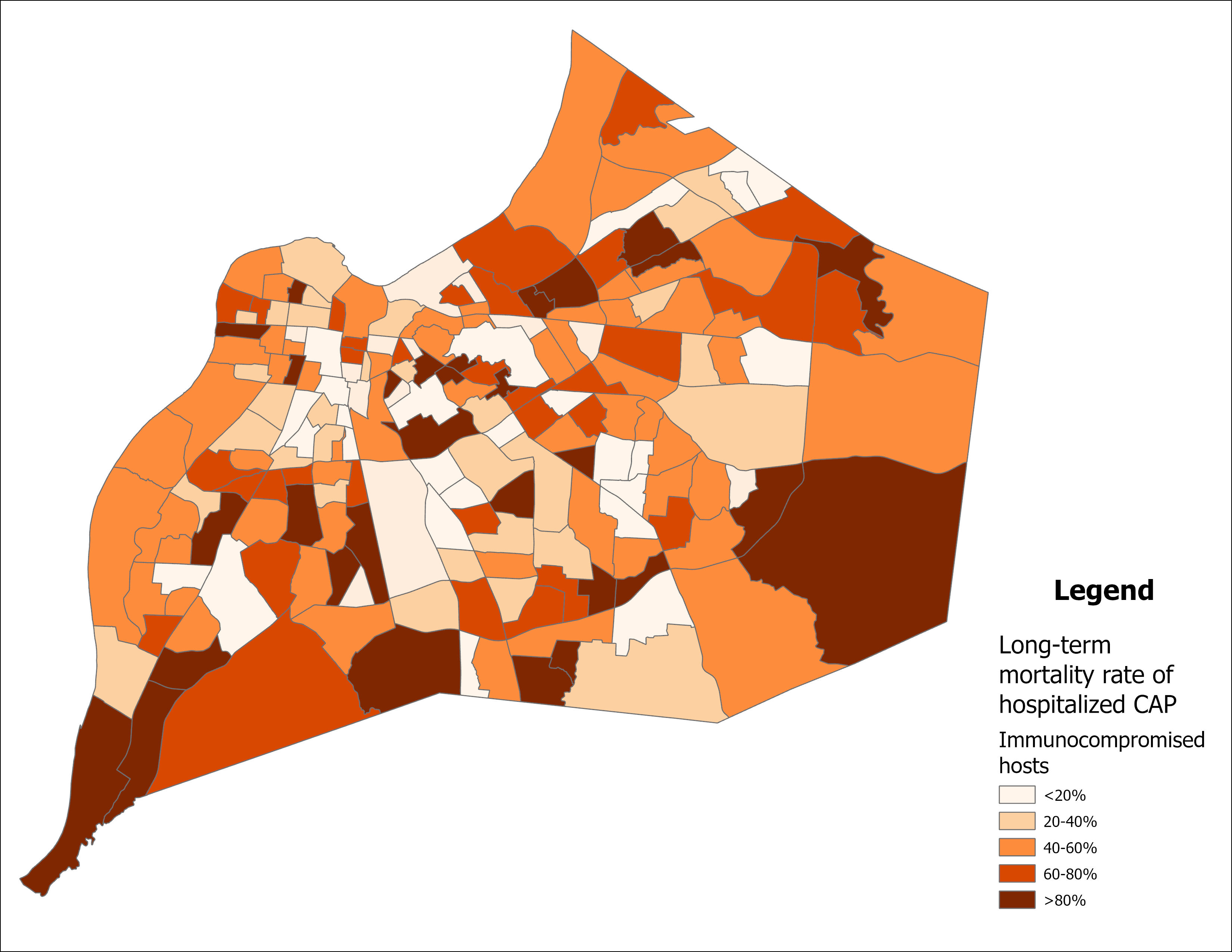
Geospatial analysis depicts no identifiable geospatial trends in mortality for the full population of patients hospitalized with CAP (Figure 5). For patients requiring ICU care (Figure 6), patients experiencing cardiovascular events (Figure 7), and immunocompromised patients (Figure 8) there were no identifiable geospatial trends.




DISCUSSION
This study indicates that incidence of long-term mortality is higher among patients hospitalized due to CAP compared to patients hospitalized for other medical reasons. Long-term mortality was close to 30% for hospitalized patients with CAP, indicating that approximately 3 in 10 patients hospitalized due to CAP may die within 1 year of hospitalization. The mortality for patients hospitalized not due to CAP was approximately 20%, indicating a difference in mortality of approximately 10%. These data are similar to a prior study evaluating elderly patients hospitalized with CAP.4 The authors reported a 1-year mortality of 40.9 % for the elderly patients hospitalized with CAP and 29.1 % for the hospitalized patients without CAP, indicating a difference in mortality of approximately 11 %. The total decreased mortality seen in our study for patients with and without CAP is most likely due to the inclusion of all adults aged 18 years and above.
Our study also found variance in mortality rates based on special populations. Patients requiring admission to ICU as well as patients developing cardiovascular events during hospitalization suffer increased one-year mortality. These data suggest that patients with more severe CAP may be at higher risk for long-term mortality. Conversely, we identified that patients who reach clinical improvement during the first days of hospitalization are less likey to suffer from long-term mortality.
In our study we defined that as the patients’ immune function decreased from normal, to abnormal, to compromised, and to severely compromised, the incidence of long-term mortality increased. Immunocompromised patients are considered to be at high risk for the development of CAP. Our data suggest that these patients are also at high risk for long-term mortality after an episode of CAP. Additionally, other CAP studies have found that a fever is protective of long-term mortality.12,13 A fever may indicate an adequate immune response to infection, thus, a lack of fever may be a sign of immune deficiency.
In hospitalized patients with CAP increased age is associated with increase number of comorbities. We previously evaluated the role of age and comorbities in short-term mortality in hospitalized patients with CAP.14 In the current study we documented tha age and comorbidities are also associated with long-term mortality. As patients became more comorbid, incidence of long-term mortality increased. Similar to our findings, staking of comorbidities have been reported as a risk factor for long-term mortality in patients older than 50 years of age in a French cohort.15
In a prior publication our group defined a geospatial association of risk for hospitalization due to CAP located in areas of the city of Louisville where African American or low income populations reside in greater concentration.10 In the current study we failed to define any association of long-term mortality with any particular area of the city of Louisville for all hospitalized patients as well as for special populations.
In conclusion, our data add to the body of literature indicating that patients suffering an episode of CAP are at increased risk for long-term mortality, but risk for mortality is concentrated in special populations of patients with CAP. Clear characterization of the population at risk for long-term mortality can help to concentrate research strategies to improve survival in these high risk groups.
ACKNOWLEDGEMENTS
We thank all the members of the University of Louisville Pneumonia Study Group that collaborated in the initial parent study.